



































Leipzig live case Thu 08.30 LINC 9.6.22 - Antegrade Retrograde combo technique






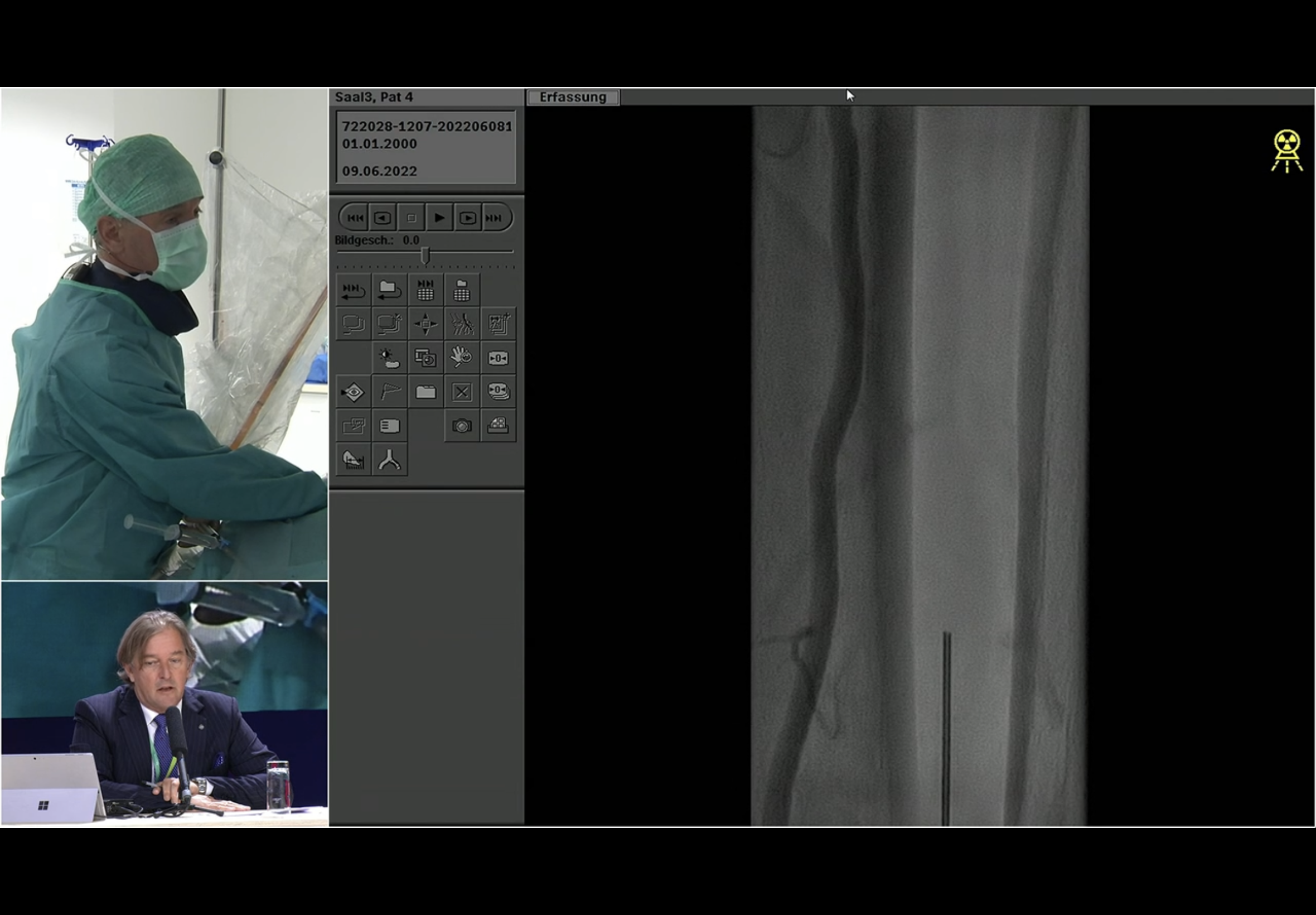
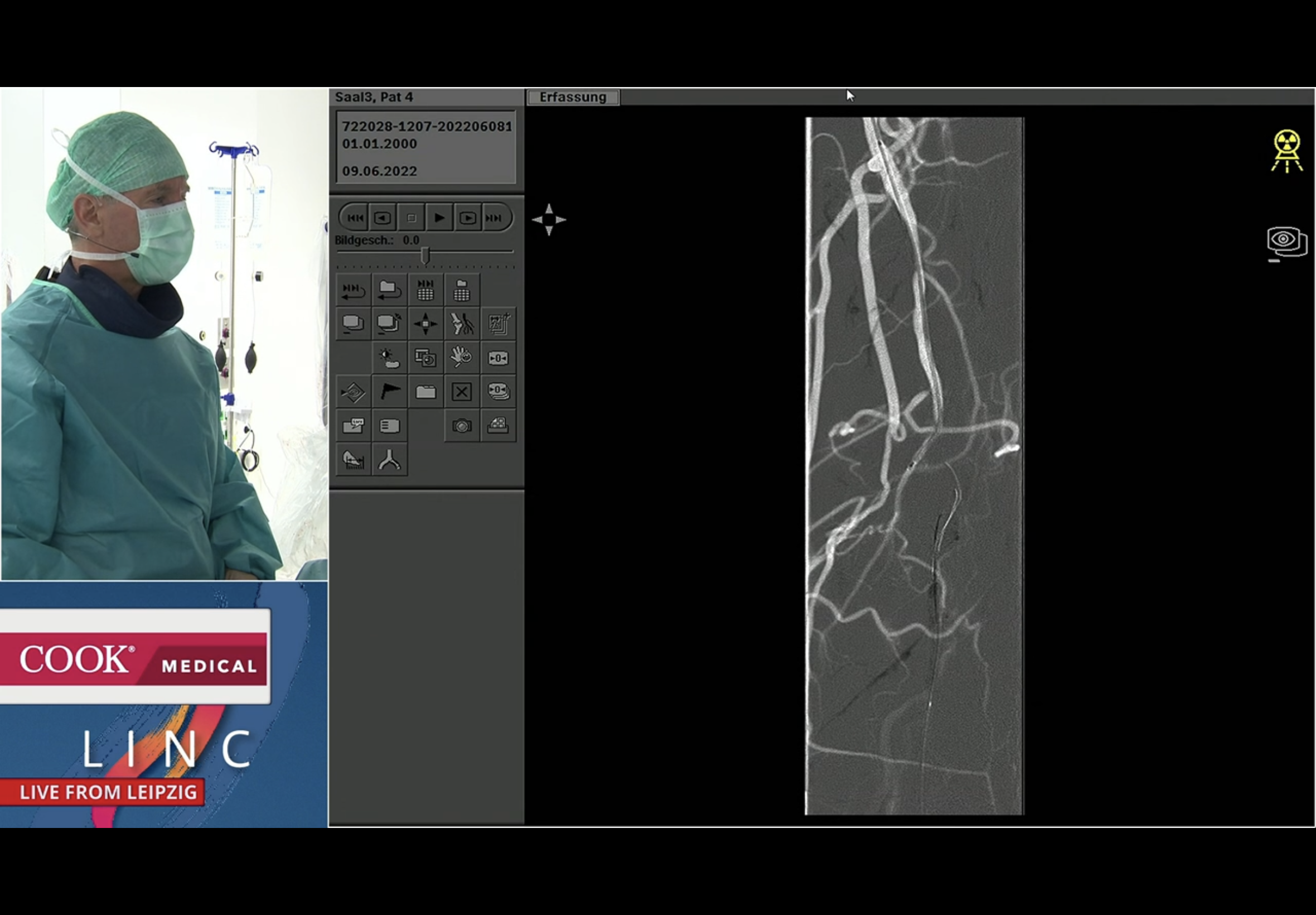
Andrej emphasises the long pop occlusion, the plentiful collaterals and - he points out - the shadow of the native vessel just about visible





It is mainly the PTA that fills - but the origin is not seen. Andrej points out the PeA on this filling. He chose the PeA for his retro distal access on the basis seemingly that the PTA origin was not clear… ? I have a feeling it was more that he wished to demo the PeA puncture technique!


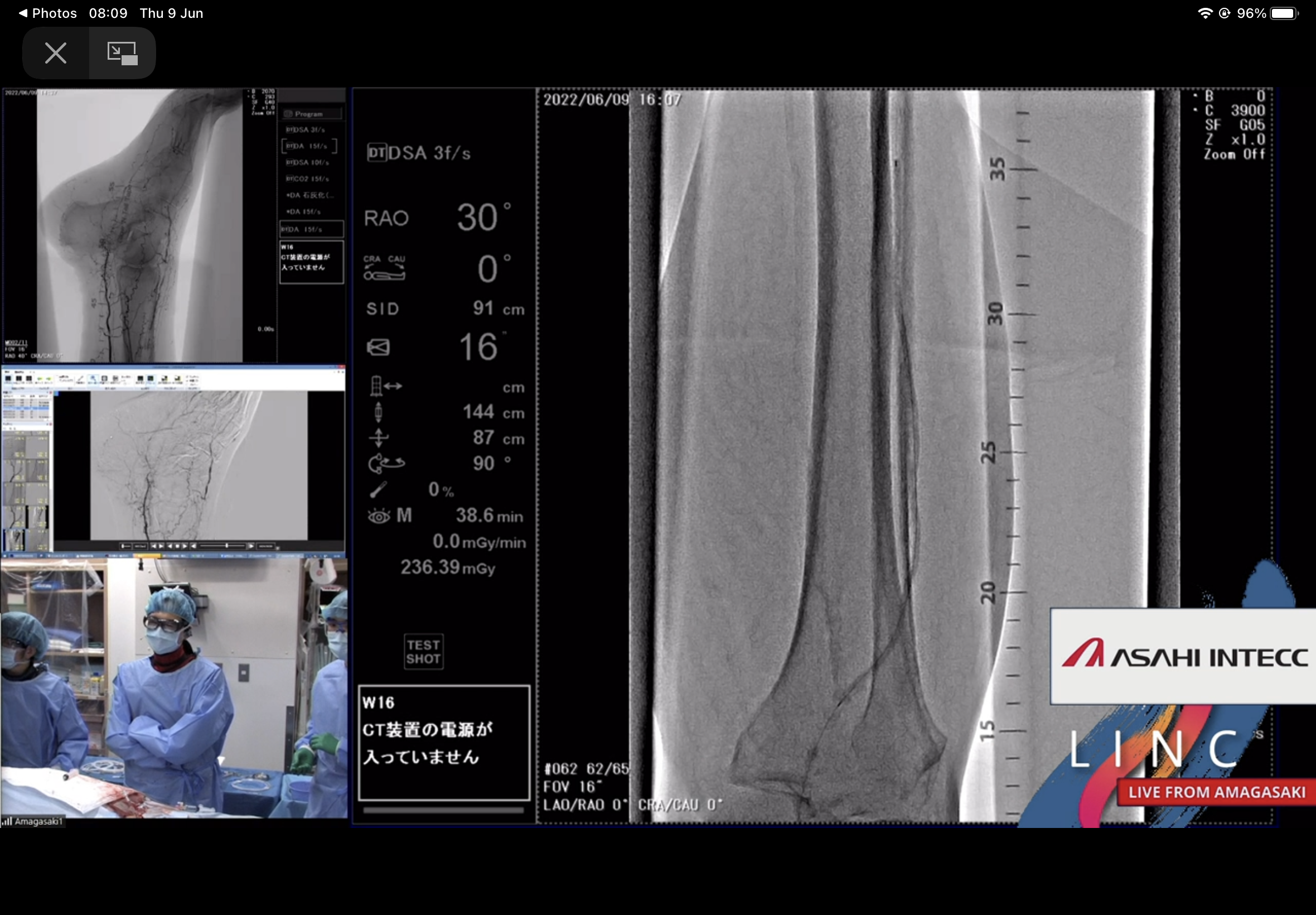
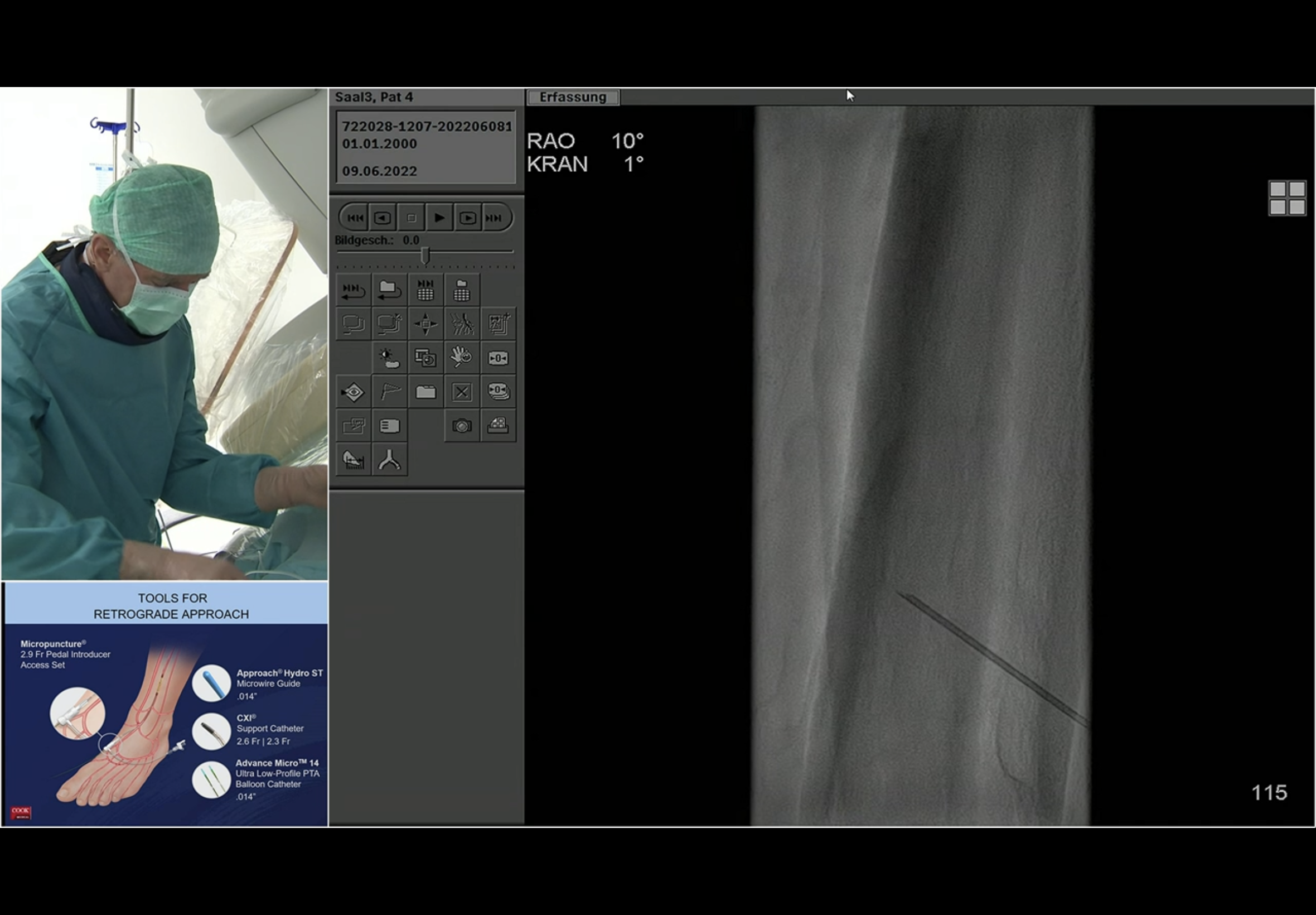
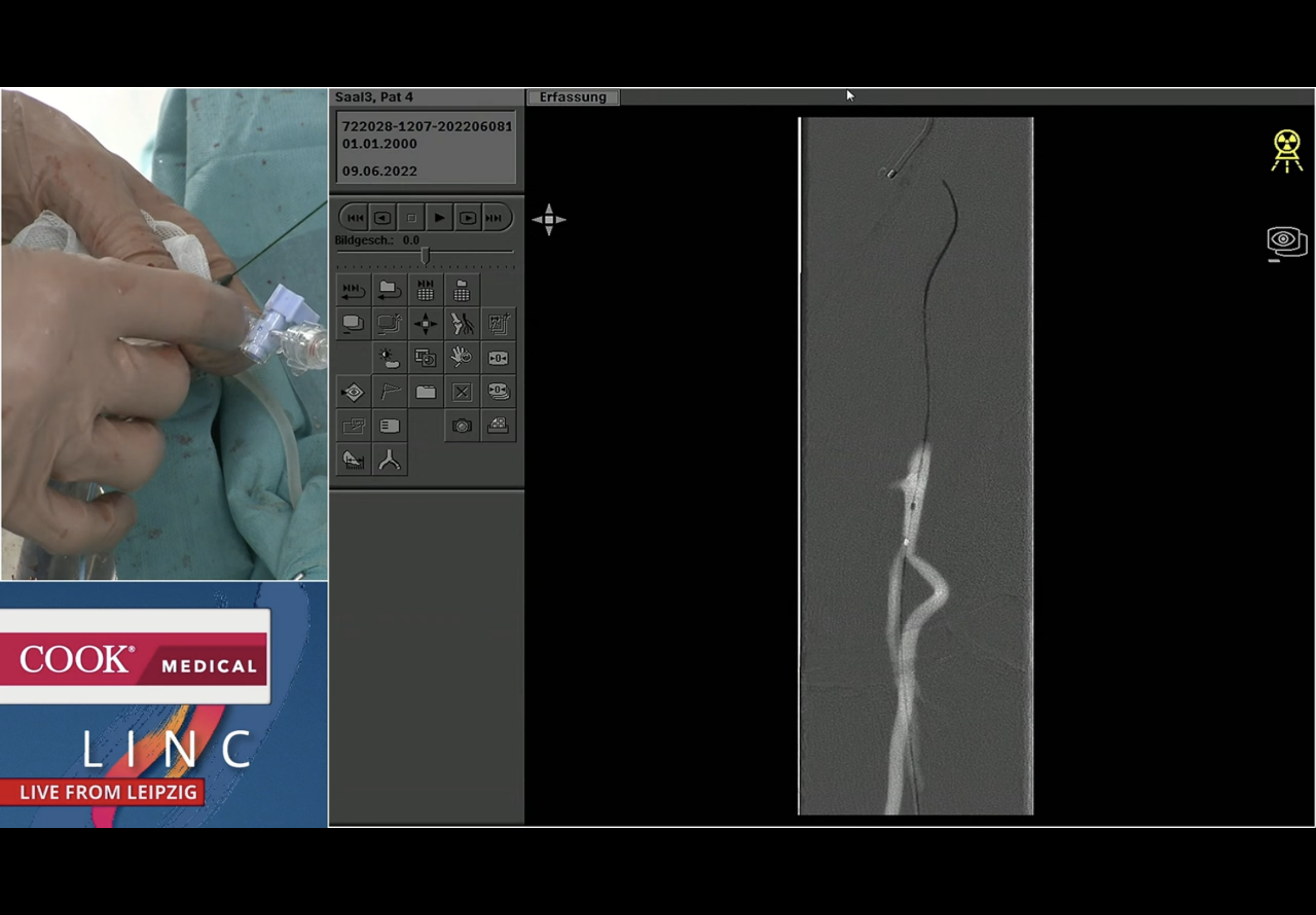
Fluoro roadmap guided puncture of the PeA. The seen vessel here is the PTA. Andrej emphasises that needle path should be parallel to the target vessel. He states that the approach to the vessel is “anterior”. The C-arm looks to be in an ipsi oblique - this is the left leg and the angle is LAO 29 on the image just before the magnified view with the needle; that is the impression I had at the time too. He then reverts to a contralat oblique RAO view to corroborate needle position and entry and then continues to work in that view.



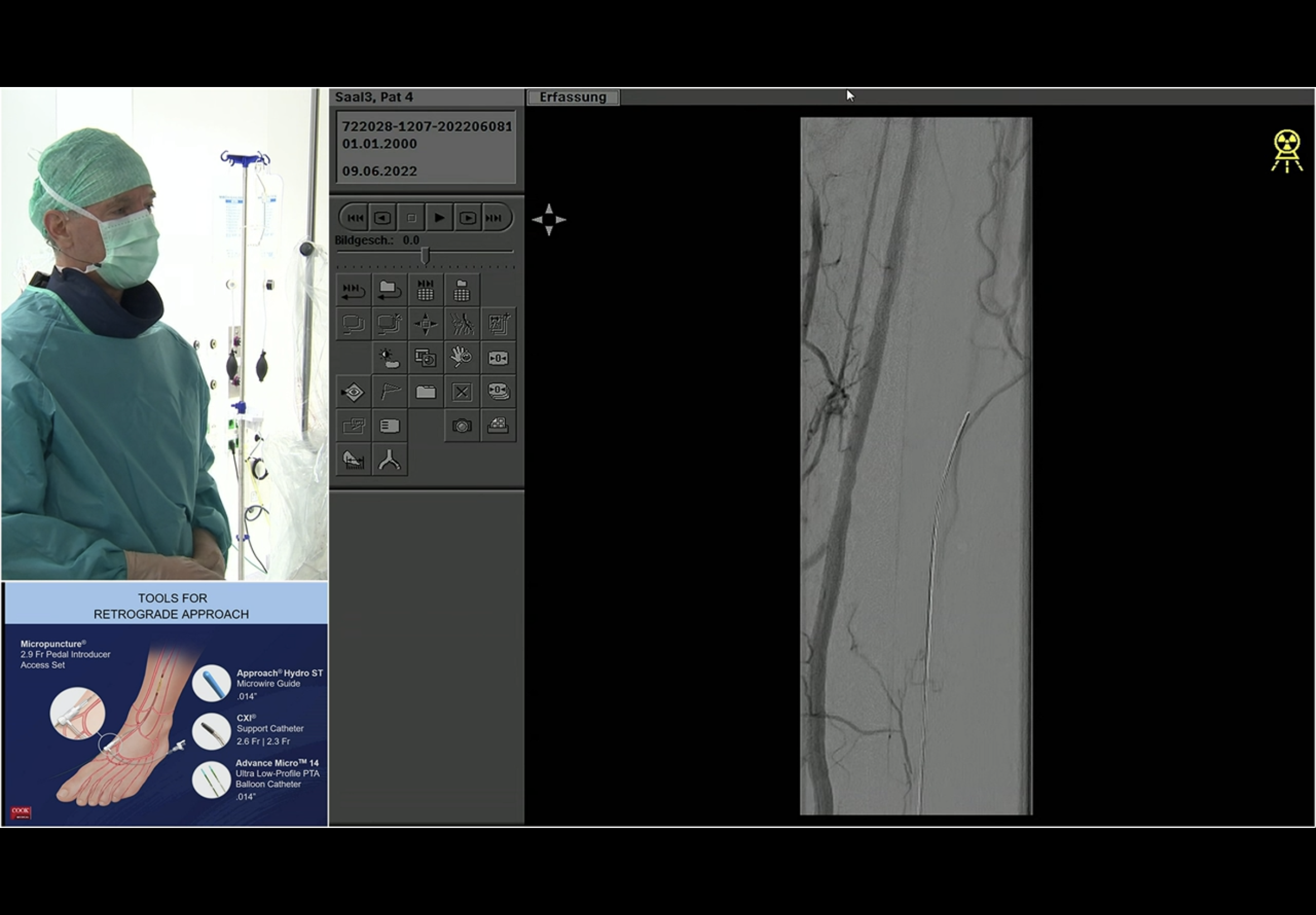
He does the next DSA to confirm for certain that he is indeed in the PeA and not the PeV; the PeA is seen outlined lightly but certainly overlying the wire coming up from below.

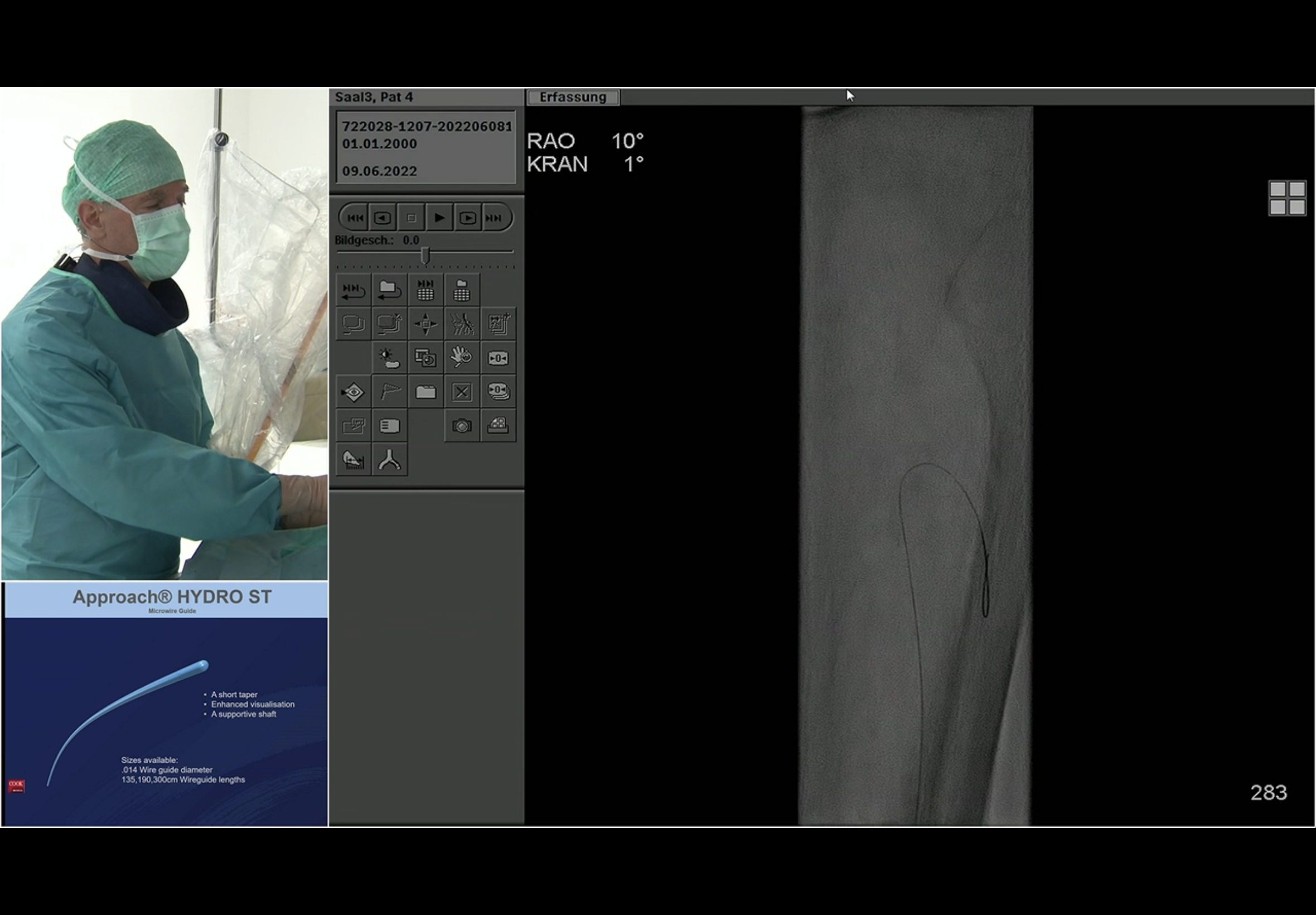
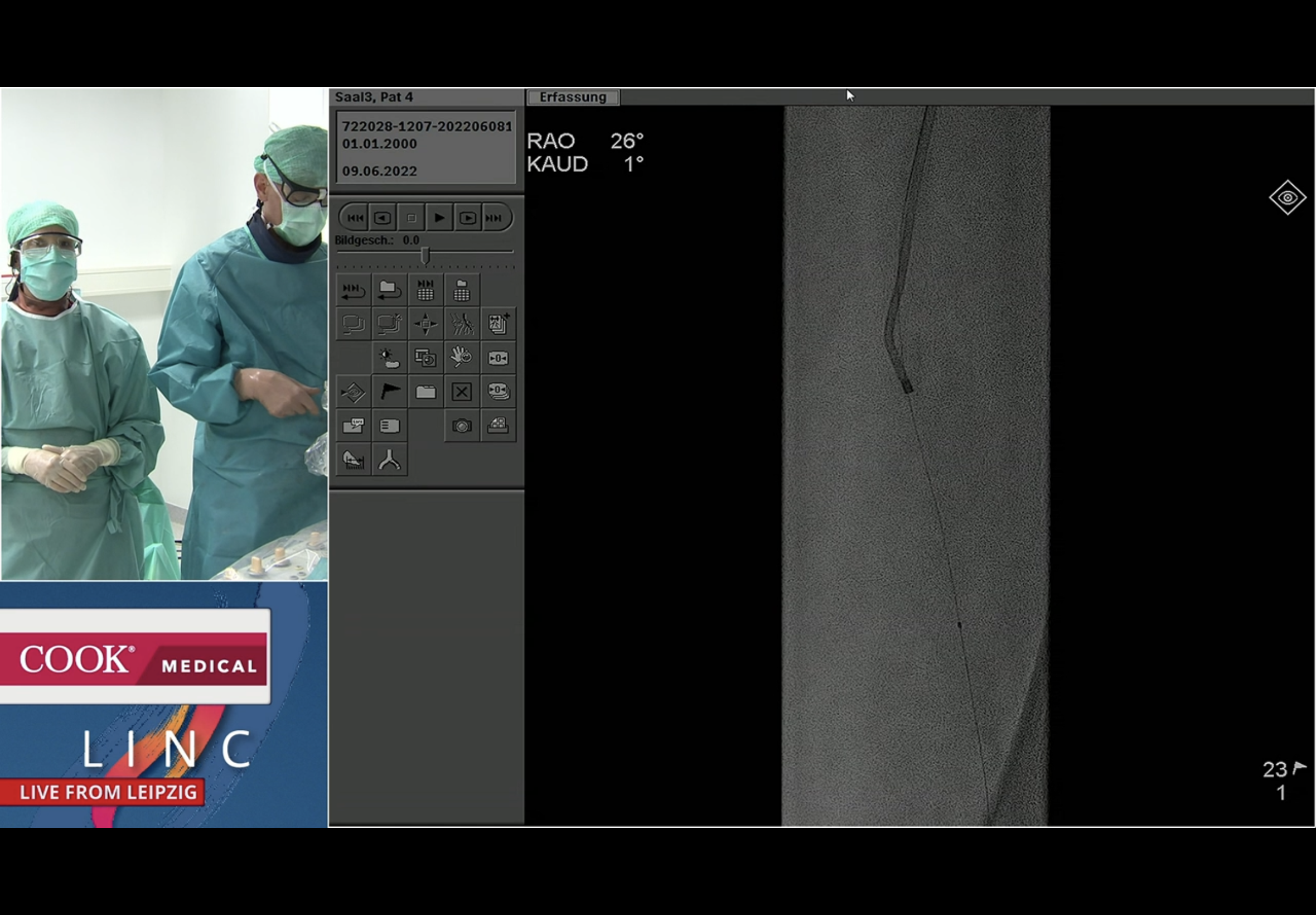
The wire going up the PeA from below first turns laterally out into a collateral; then it turns medially and Andrej susses that it may in fact have gone into the PTA origin.



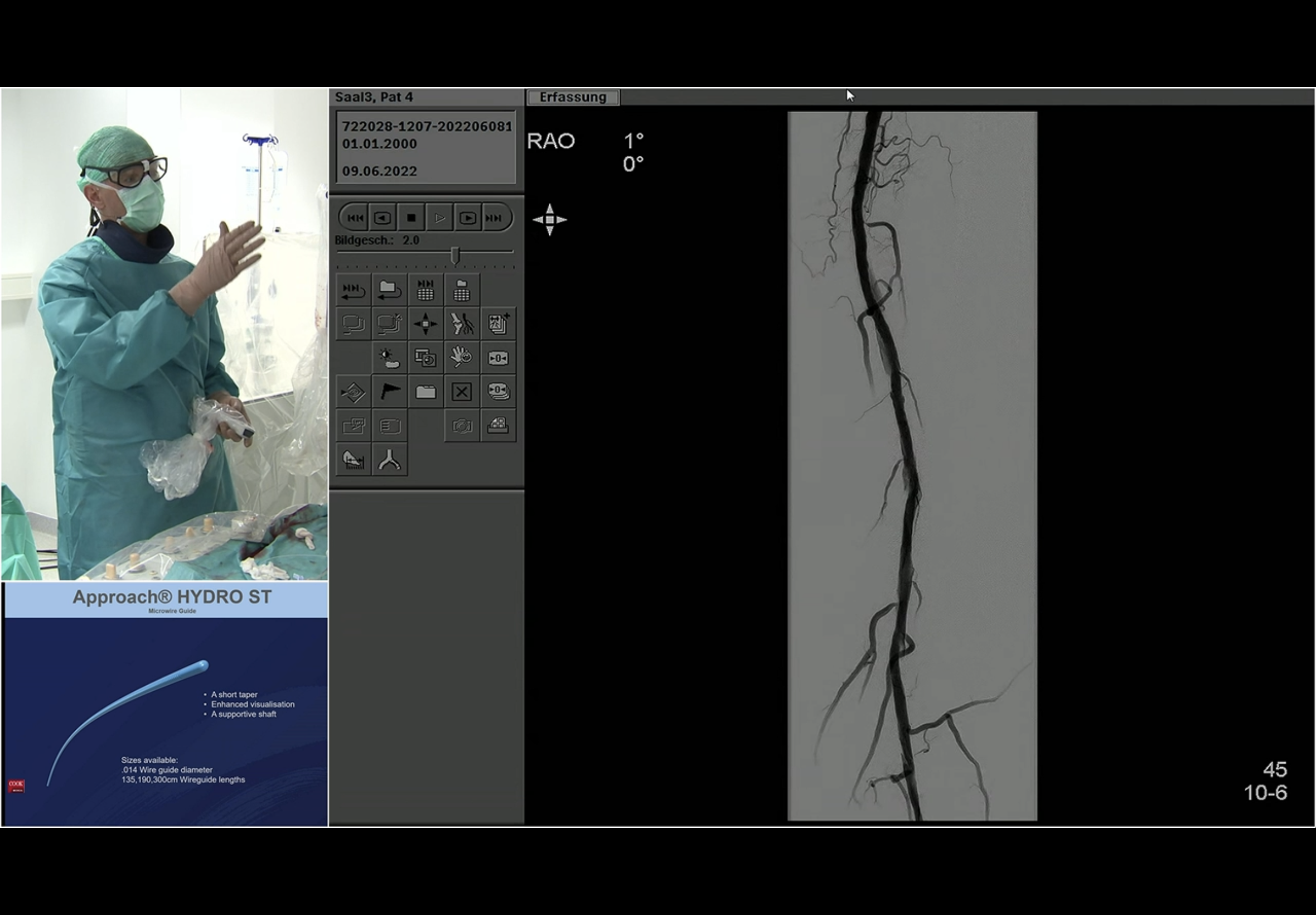
So he then decided it made sense to go ahead and balloon the proximal PTA up and over from the retro PeA approach! As you do : - )























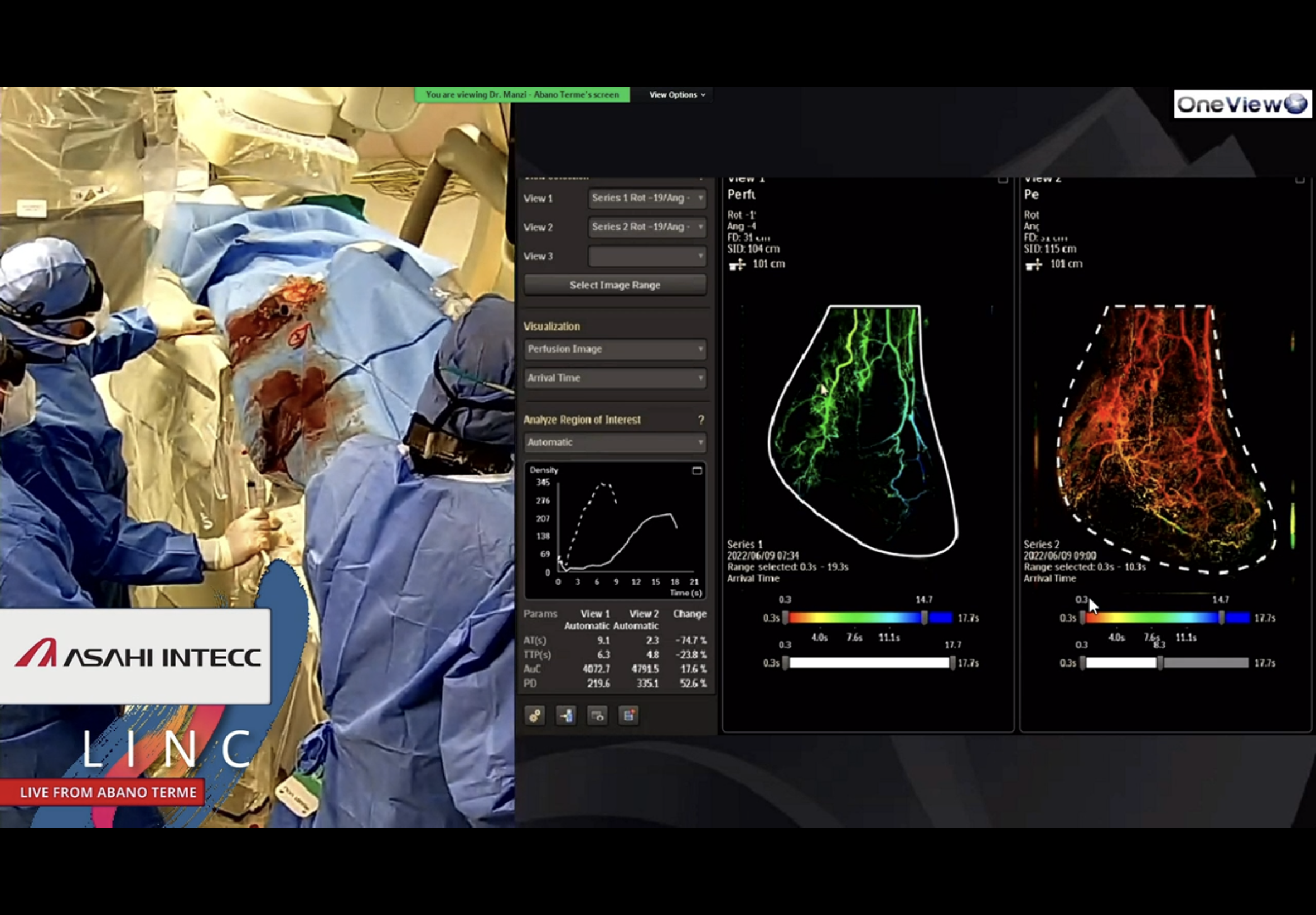
Manzi live case - 08.15 Thu 9.6.22 - CLTI TMTA stump






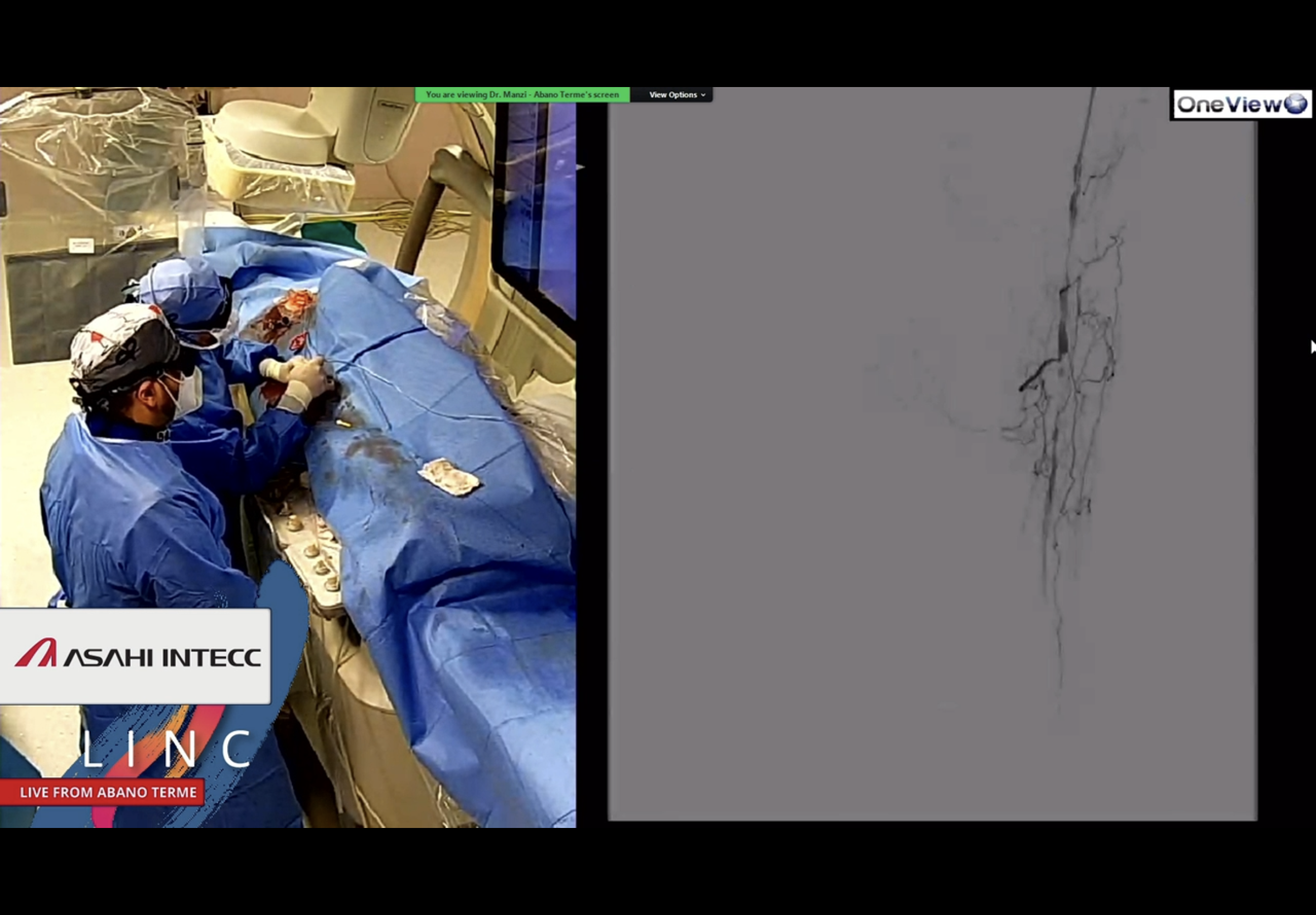

The point at which Ferraresi asks Manzi - What, pedal plantar loop again!?













Ferraresi talk Asahi session Thu LINC 9.6.22 - Status CLTI

RF introducing the Japanese session last day LINC 2022 first on day































Andrej Live Case - NOT kissing.
A few DSAs from an example of Andrej Schmidt treating a right CIA CTO flush without a stent on the patent left CIA.
From Tuesday 7th June 2022 at LINC.


At this stage Andrej and the panel both agreed that he was just a fraction too short for this to work.


After this DSA, the moderator - I think it was Reijnen - said he would drop a mm lower; and Andrej said that he would go a mm higher (which is what he then did) !















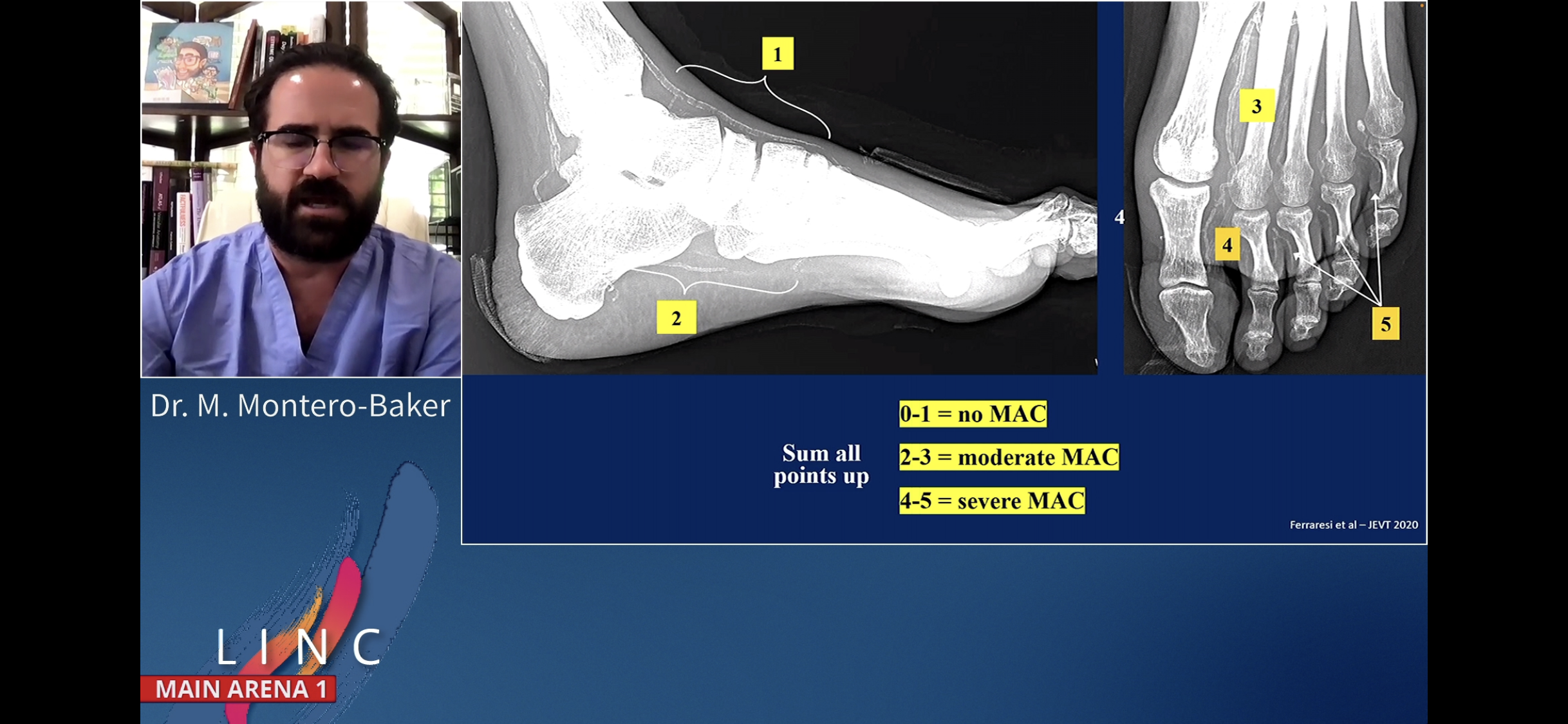
uMAC scoring for no hopers with MAC
Miguel Montero-Baker and Jill Somerset
using ultrasound MAC to triage out the no hopers on account of severe MAC













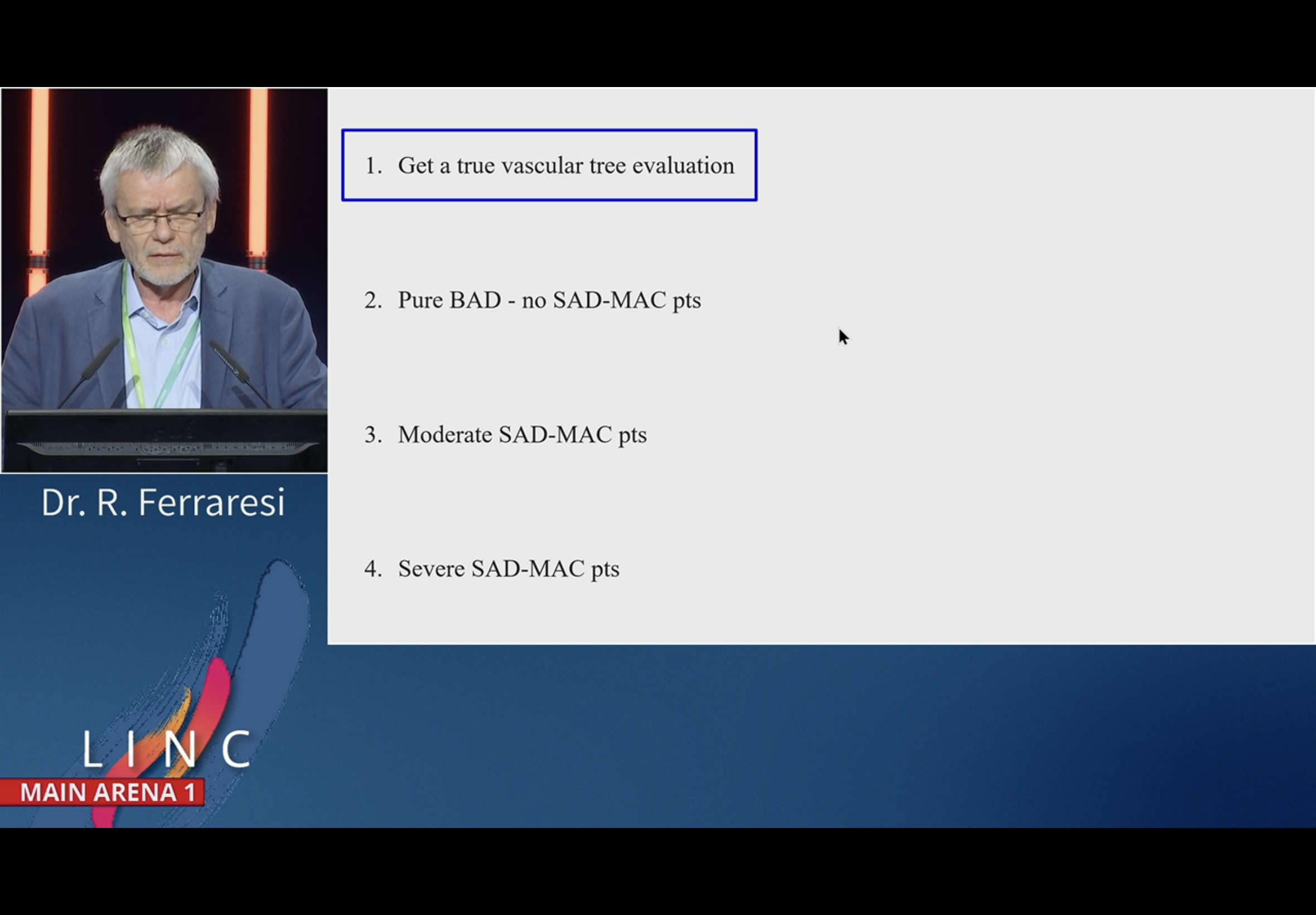
BTA disease - when not to. Ferraresi. MA1
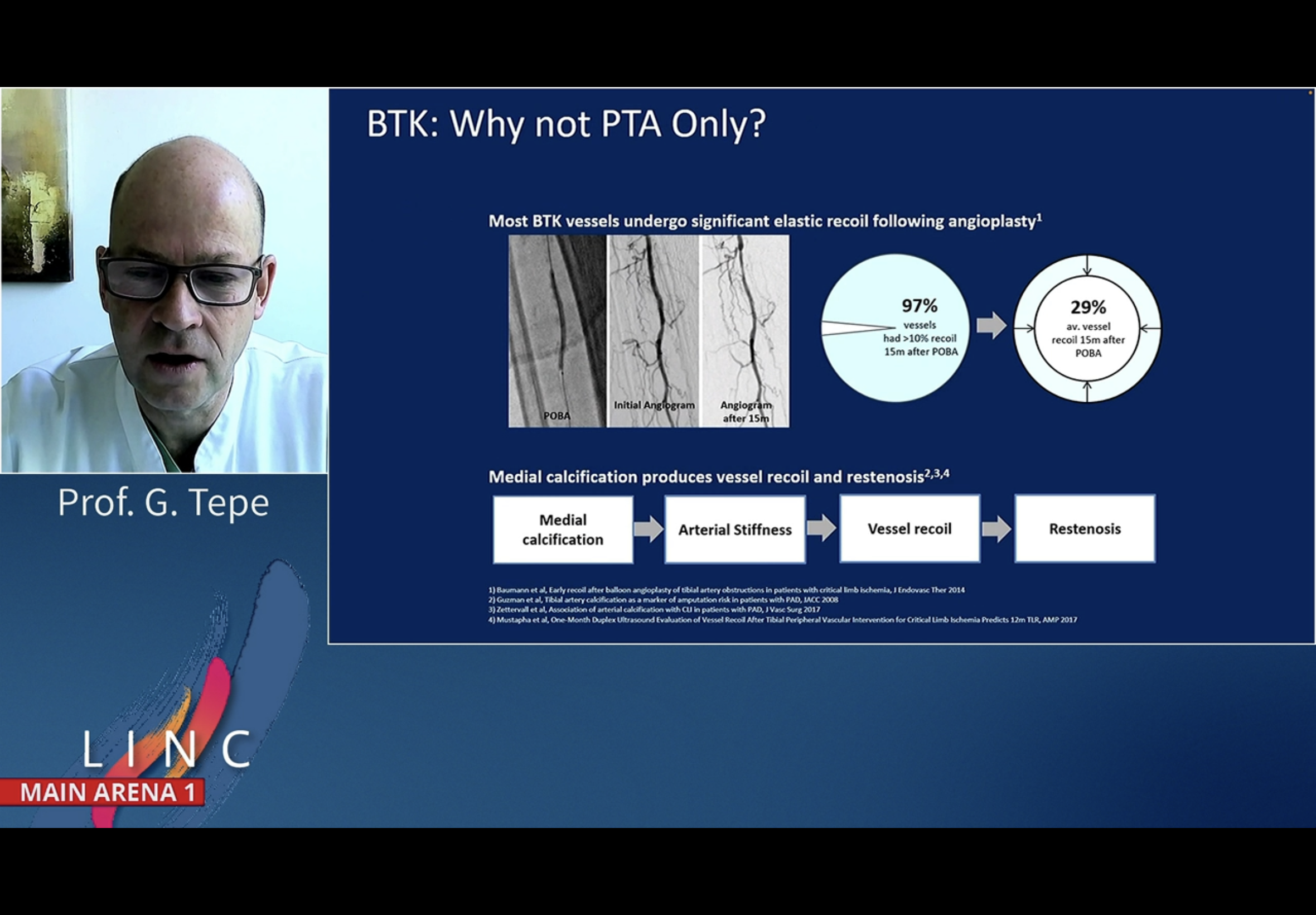
Great talk. I lost the last few slides. Essentially - for the last category with Small Artery Disease (SAD) and severe Medial Artery Calcification (MAC), be gentle and do not go all out on the aggressive endovascular measure, careful to underinflate than overinflate.





































































Jihad double. Haemodynamic v anatomical CLTI. then histopath tibial. MA1







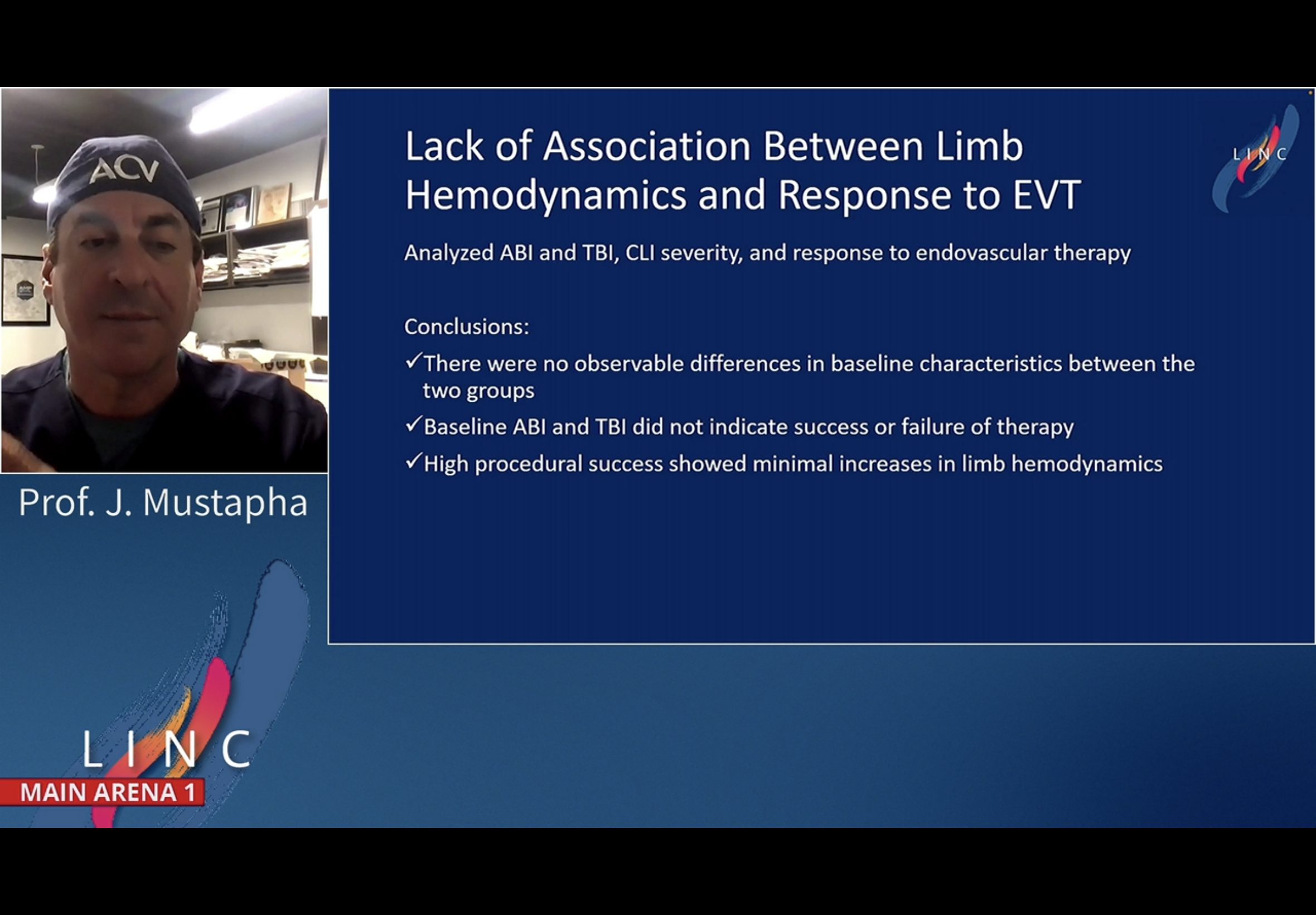








Sadly lost last few slides
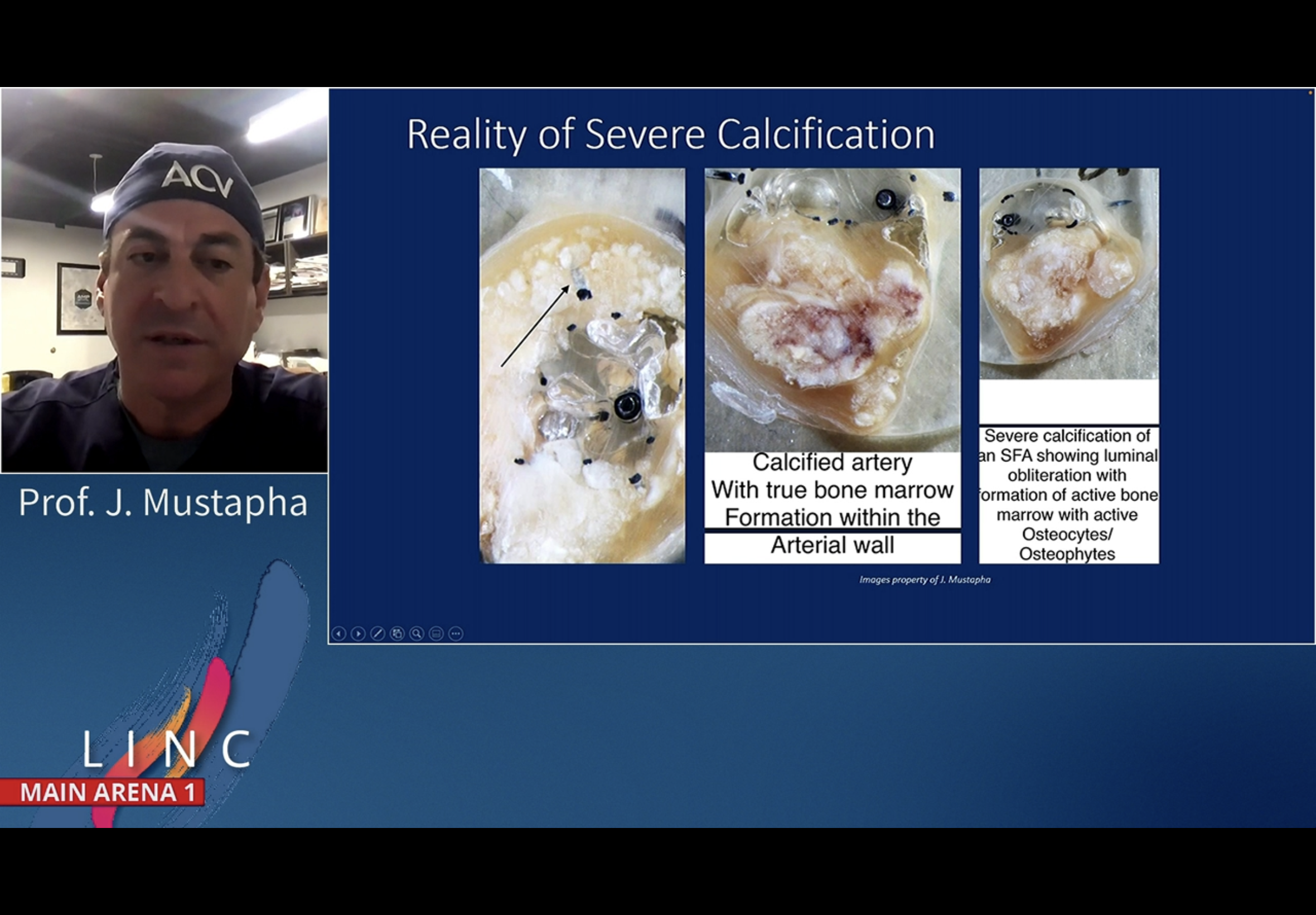
Jihad stressed five different pathologies concentrically out to in through the wall in tibials. Each needs getting through.