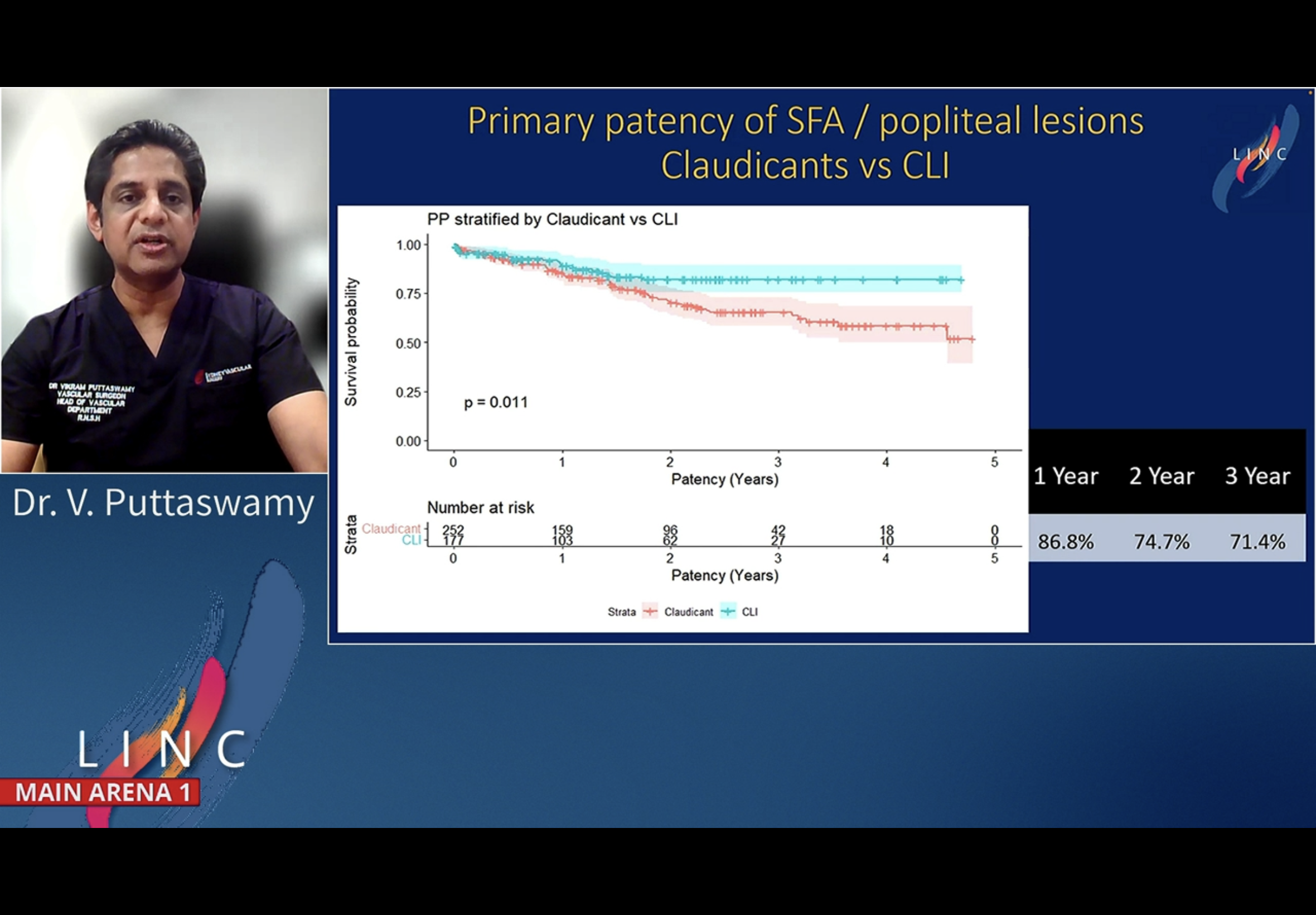
Directional Atherectomy - DA - Puttaswamy 3y data
Regsitry ste up at North Shore Aus
VP found better PP results with CLI patients than IC pateitns
PP better in larger vessels, but no diff between tibial and SFA Pop
NO distal emboi complications needed surgical inervention
No major amputation
Qn from Zeller: why differen in your study in terms of outcome at different vessels compared to other study - A: may be due difference in lesion lengths treated.


















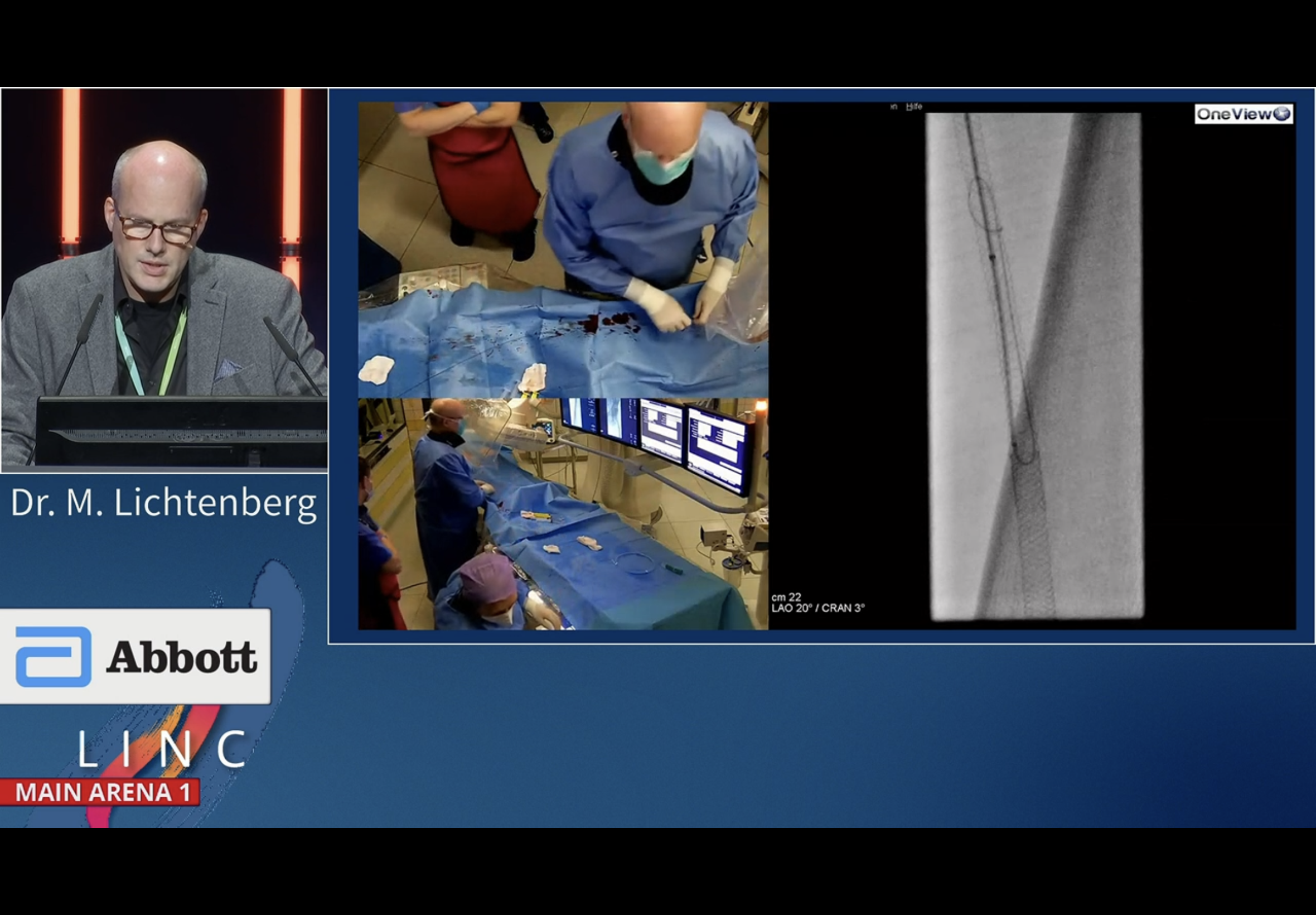
Recorded case on Serranator serration - Lichtenberg
vessel wall compliance is the main issue. Some vesle areas with very stiff hard calcium. Even broke a Terumo wire. Therefore used Go Back. Got needle into calcium. Then an 0018.
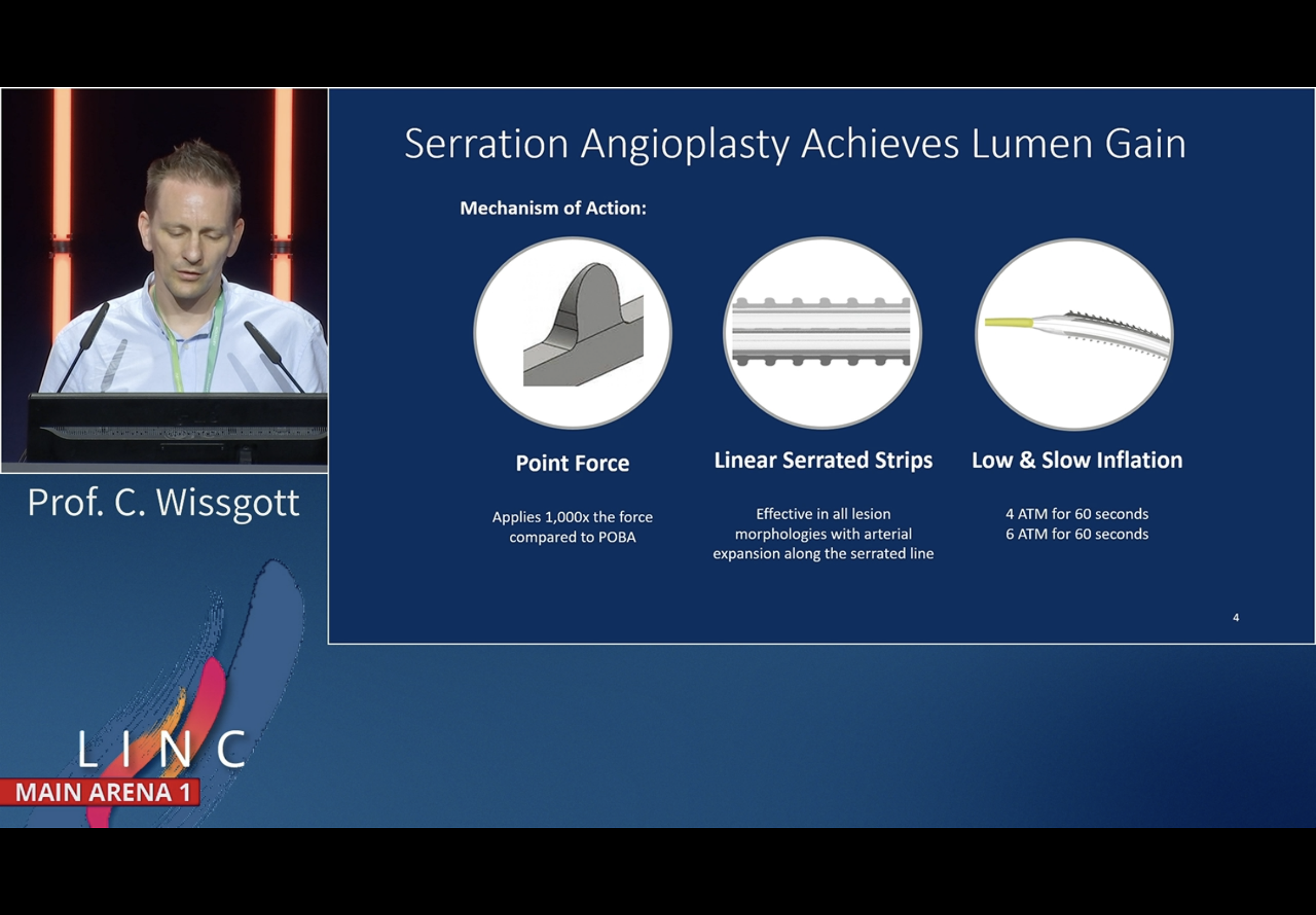
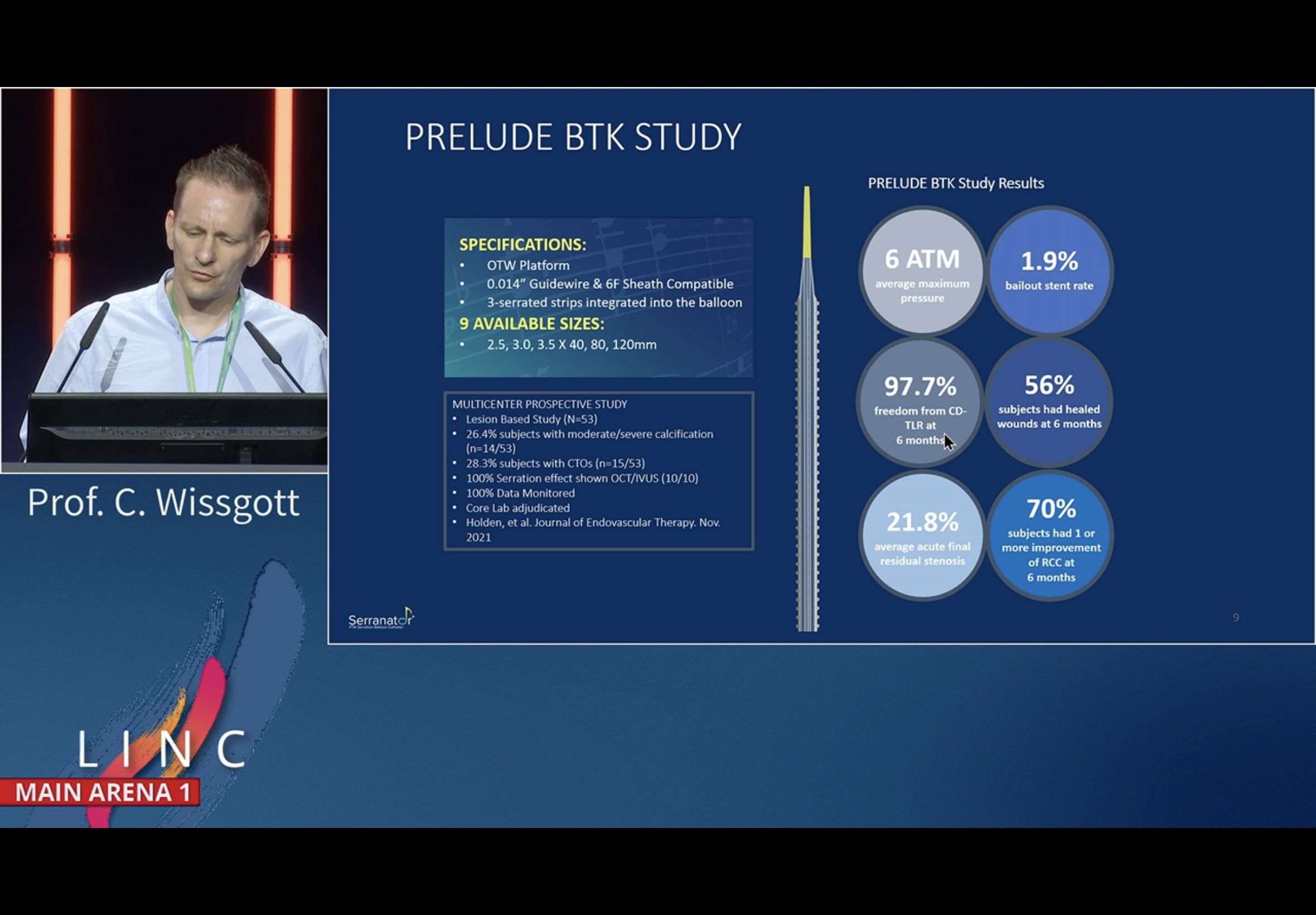
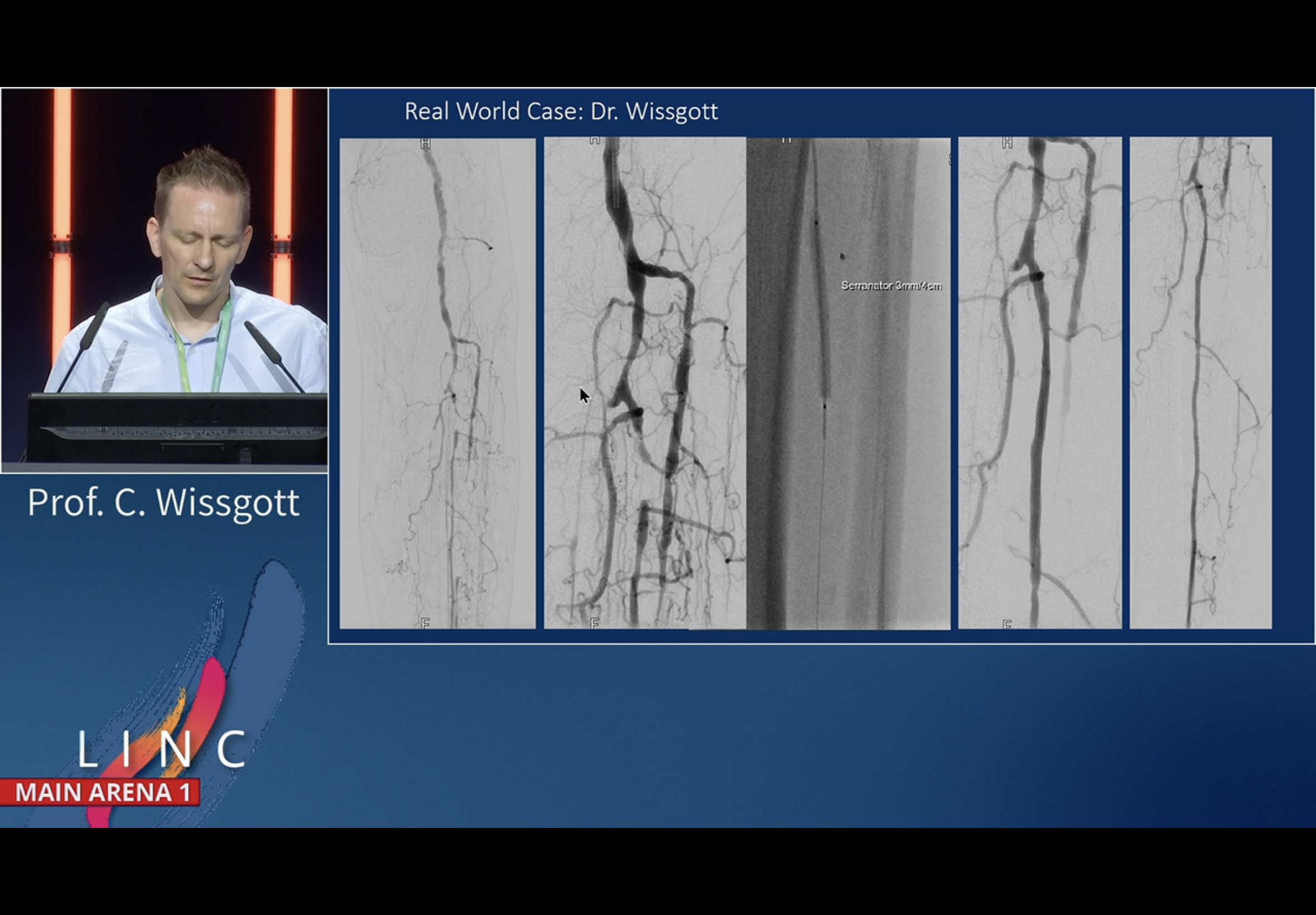
Serration for lumen gain - Wisgott
Serration allows greater directed force at lower pressures
Slow inflation
Can treat all lesion morphologies
Christian Wisgott
Even showed a case of focal non-response to atherectomy that worked with Serranator

Schneider comments - learning from dCB era that vessel prep v important.
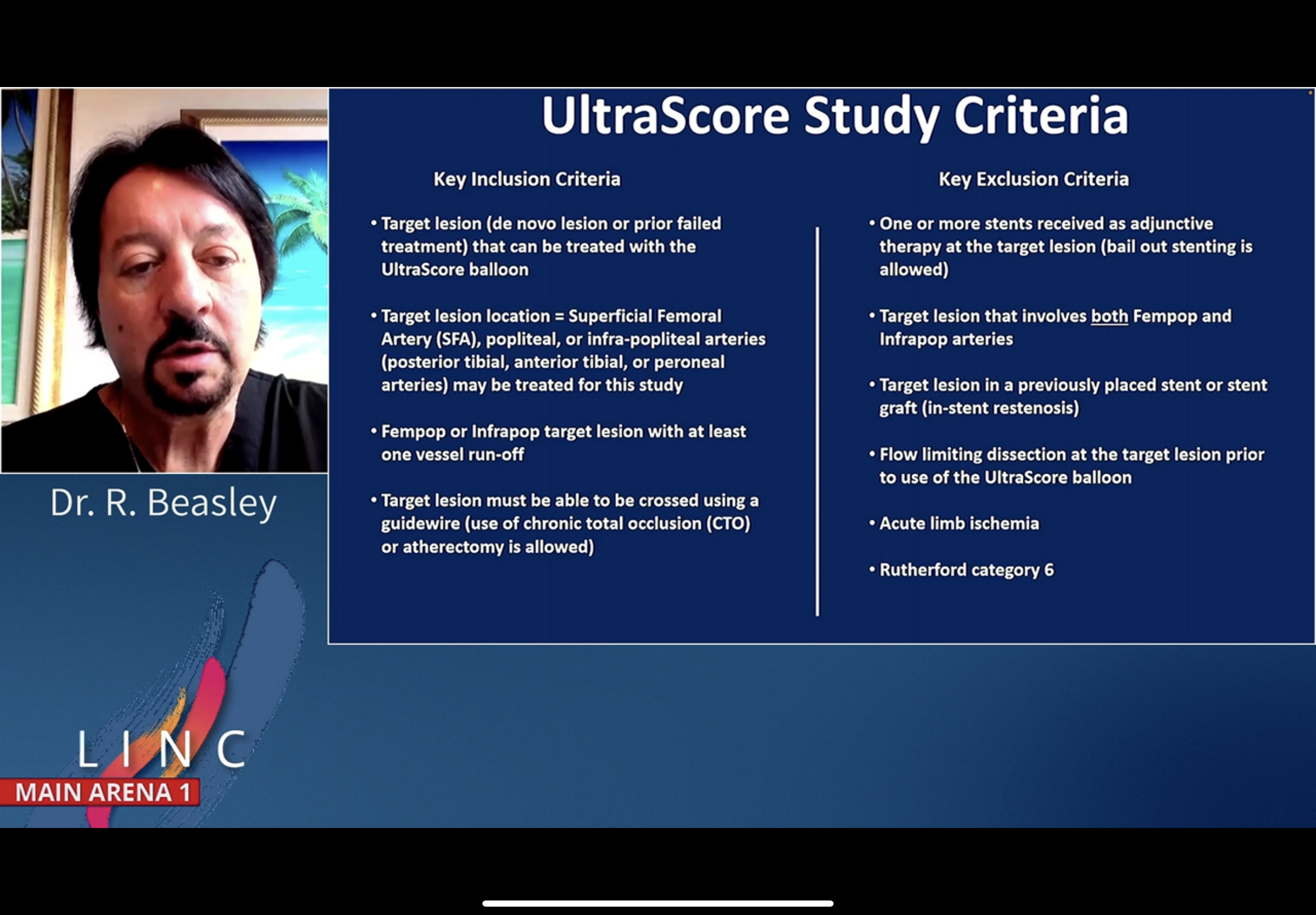
Bob Beasley from Miami agrees with what PS says. Interesting that may take atherectomy out of the picture.
Deloose - can it be definitive Rx in BTK?













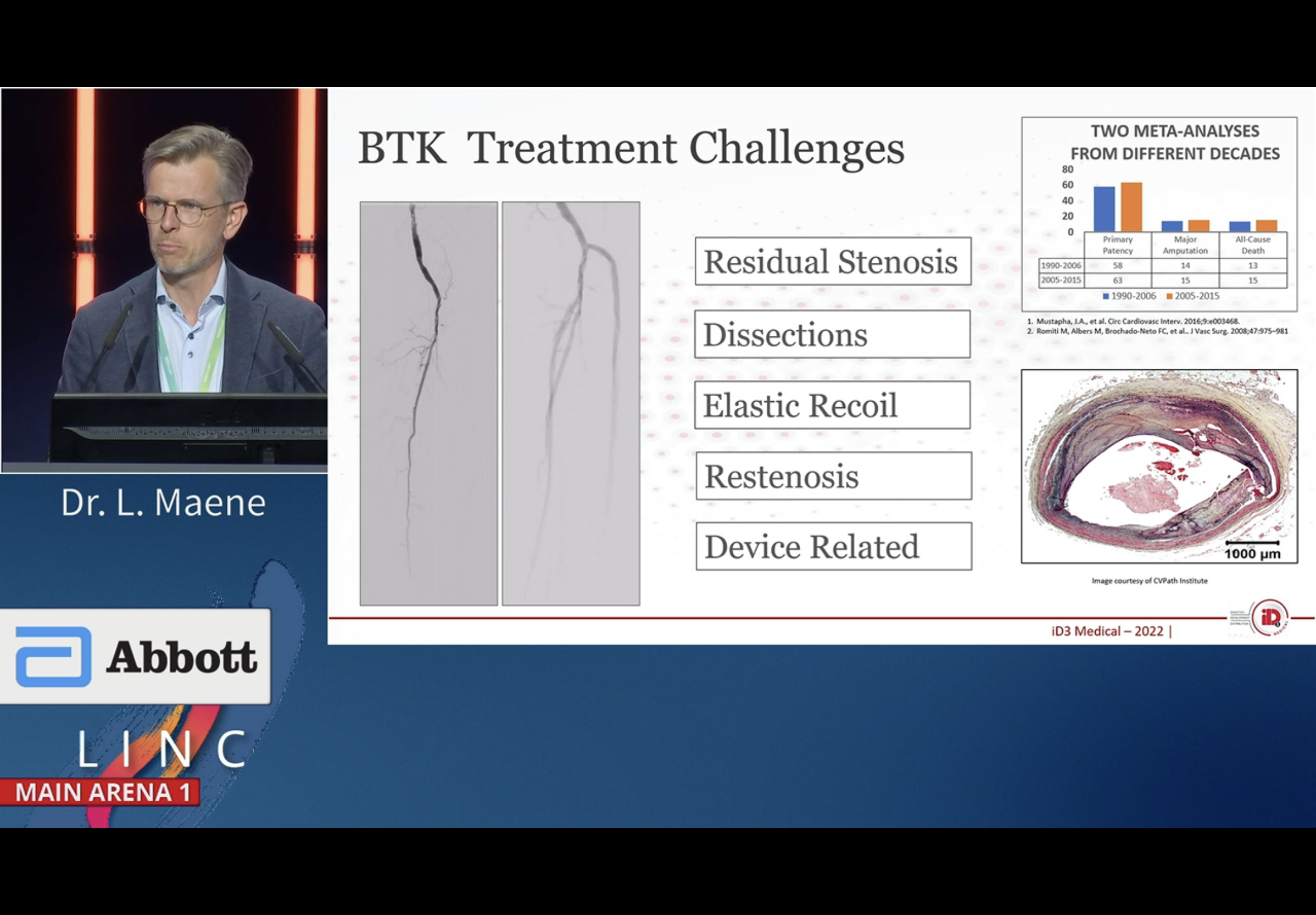
Drug eluting scaffolds at BTK - Lieven Maene
The challenges with BTK have not changed much in 2 decades.
Focus more on vessel prep and vessel check. WE were undertreating! Underestimated the diameter BTK.
Also were underestimating the exten of dissections.
Changed approach - incorporated vessel check. Extravascular US. Built into the machine.
Need scaffold. Scaffolds do affect negative remodelling so need drugs, may need long term drugs.













ALI Rx with JET-i percutaneous thrombectomy
JET-i system. Israel made.
6F device for arterial 8F venous
high pressure saline pump
50m IC ED pxn
150 cm long stents SFA Pop all occluded
started with 35 wires then 0018 for the JET-i
pushablility and trackability over the 6F are very good. Even on organised blood clots. It can track through stents even without the guide wire scafoold.
Good result no signs of distal embolisation.








Questions
Comparable for arterial the Rotarex and the JET-i.
Suggests prospective trials (ML). DS says - how imporant is th pulse spray? ML - think it is… rubber-like material in the viabahn.
how much blood loss? average 150-200 mls.
ANy experience with PE so far? No.
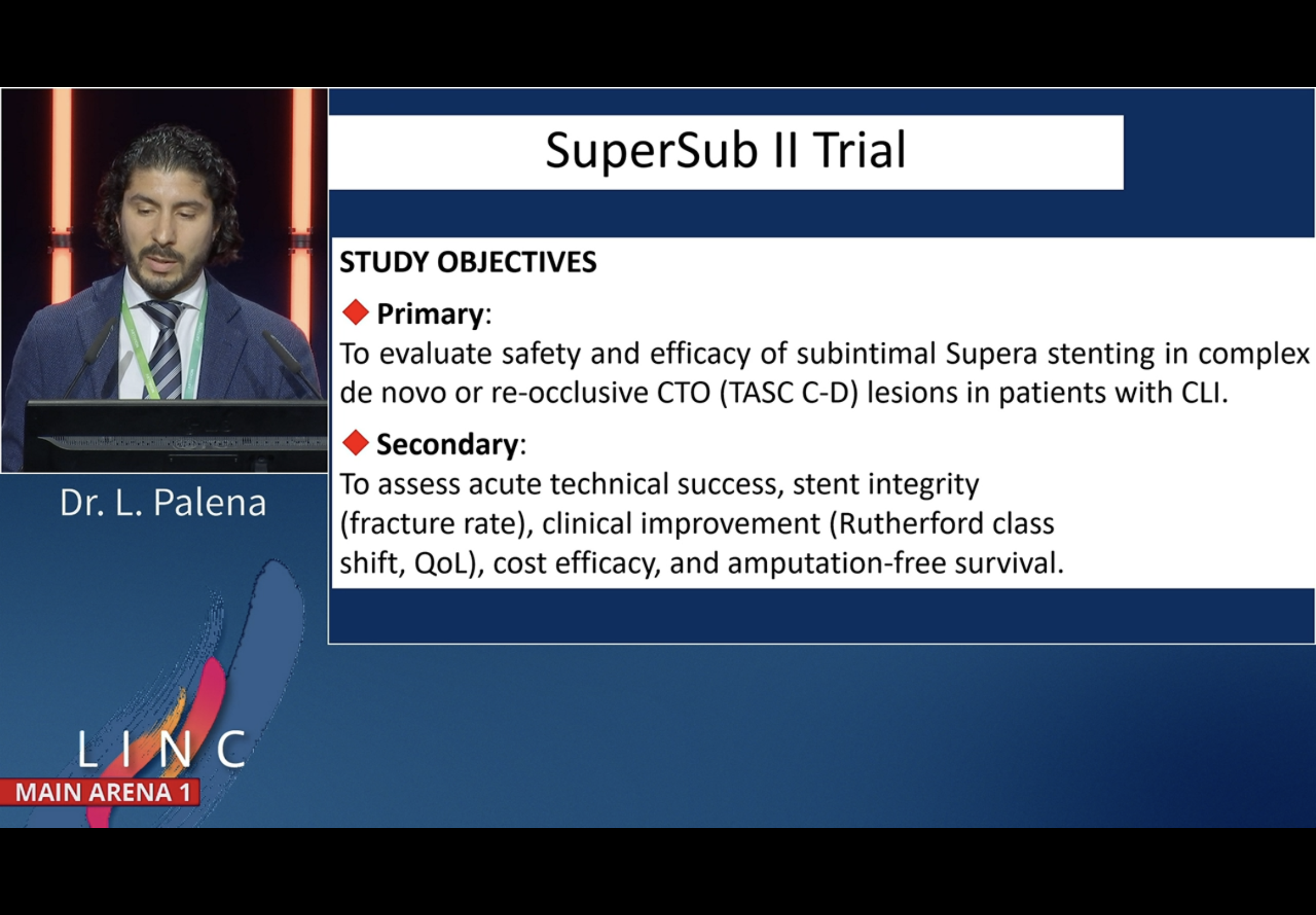
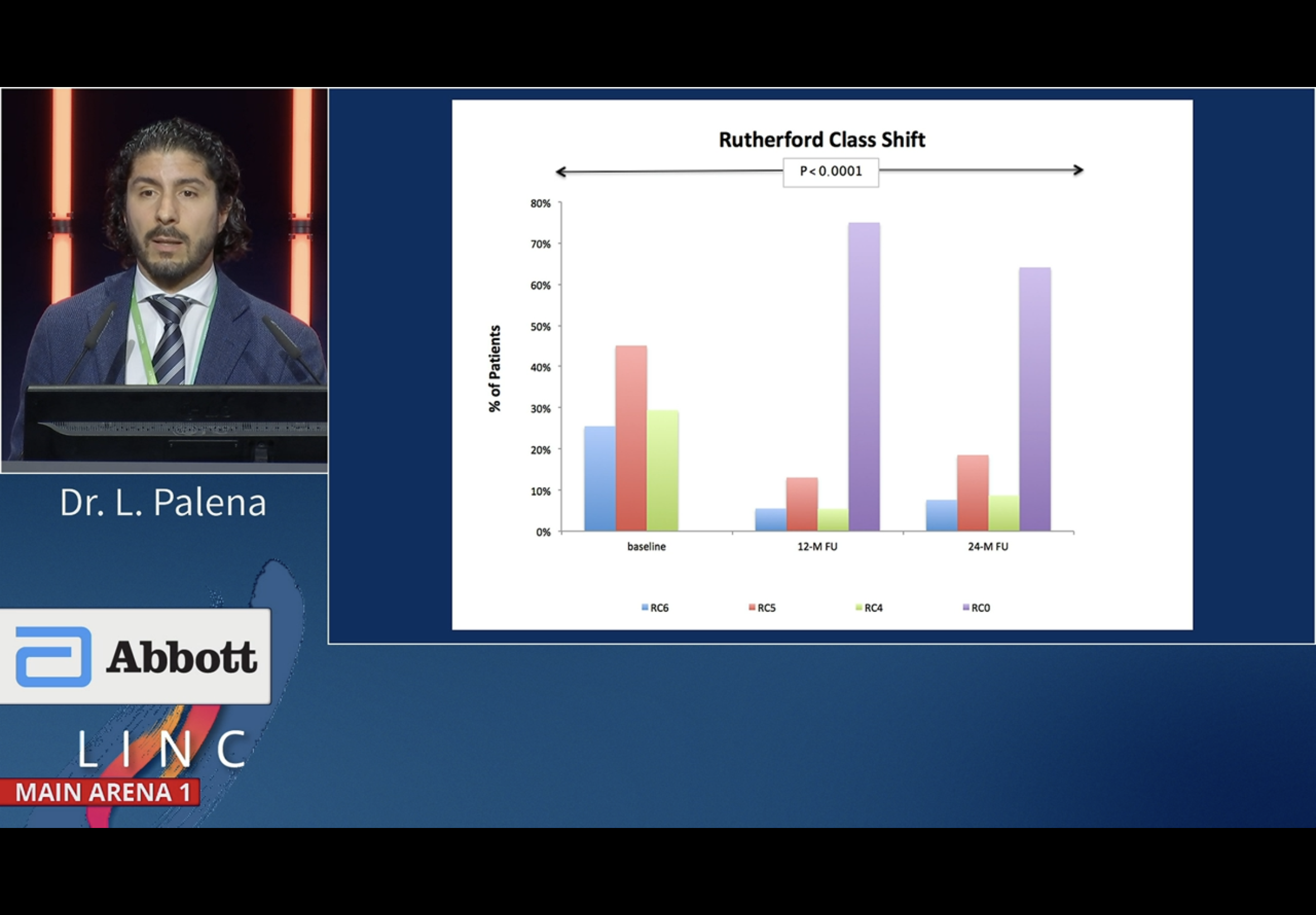
SUPERSUB - 2 yr Supera data from Abano Terms
Palena
Tasc C and D Supera study - not reandomised, observational
Correction PP was 12 mo not 24 as says on slide
enrolled 92 pts
All lesions treated were CTO
Lesion length 26 cm on average
Most reinterventions happeneed within the 1st year
The fatal MI was 5months after procedure
All pts at baseline were Rutherford 4,5,6
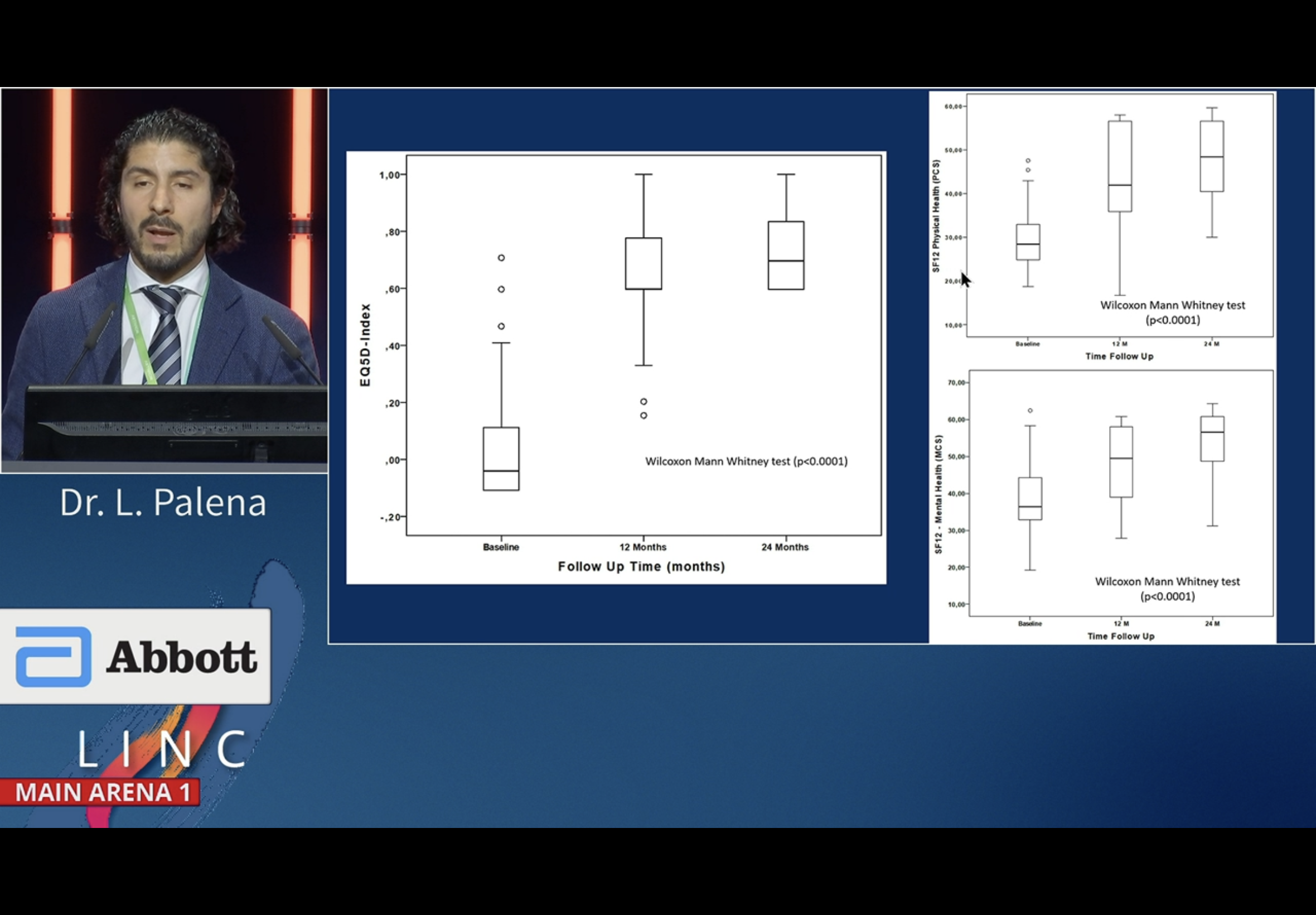
They did SF12 data too
Questions from Dierk S
Palena says Eluvia data is competitive. Difficult to compare populations. Supersub data has NO endoluminal crossing patients. Diffiutl to filter out the effect of drug elution. Difficult to compare that with the mimetic technology effect / impact.
9% comlication rate with PRESTO technique… how should we deal with the puncture holes?
We are aggressive with labelling complication. Even a pre dilation perforation is marked by us as a copmlication, such as during vessel prep.
Qn: yo used quite a few 4mm Supera?
We tried to avoid even the 4.5mm diameter … however the P3 cases perform well with the smallest one. Some other of our centres were using 4mm.
How many stent occlusions in FU (DS)? Comparing freedom from TLR and PP there is not much difference. Have the percentages not the exact number…Not many.














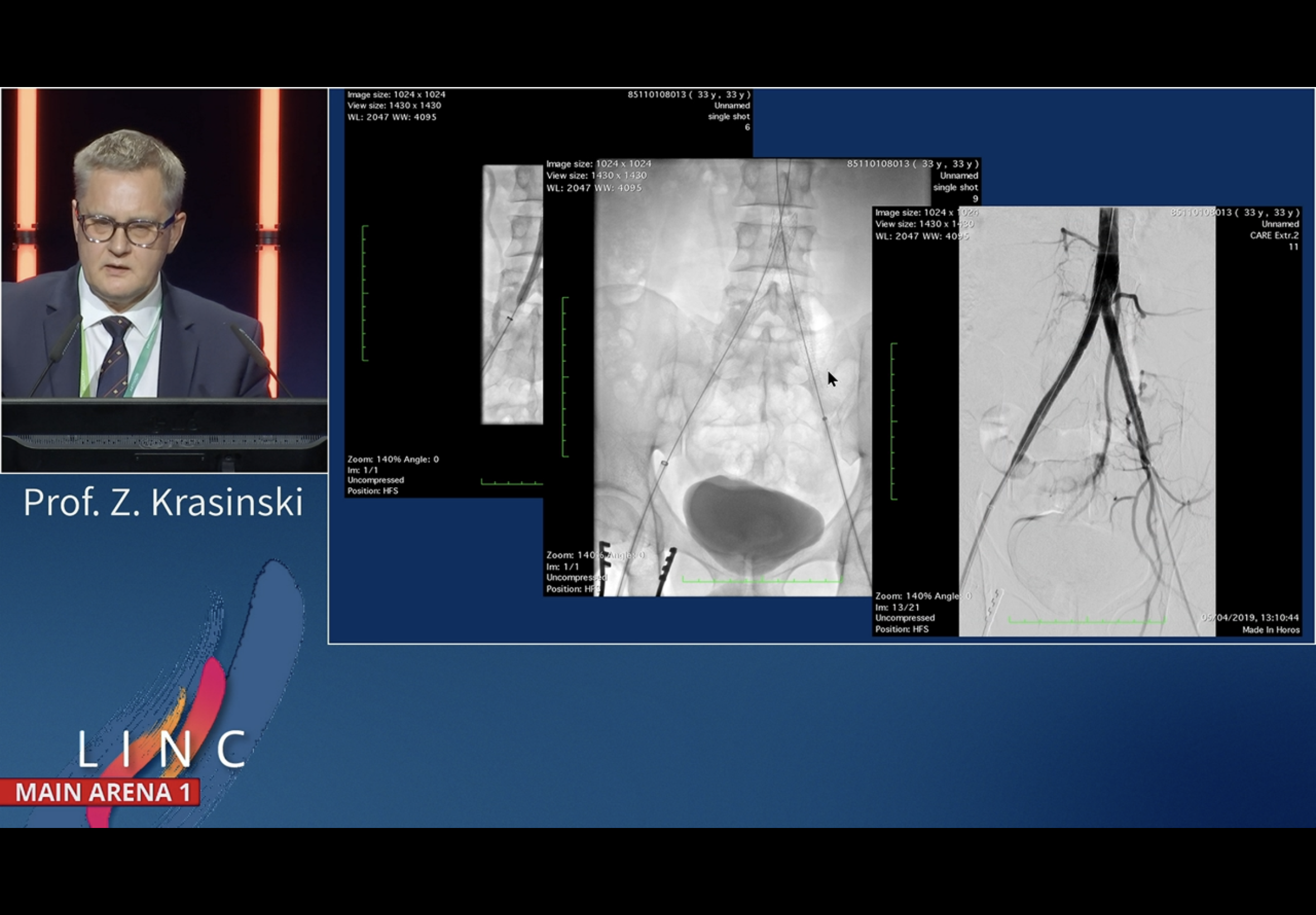
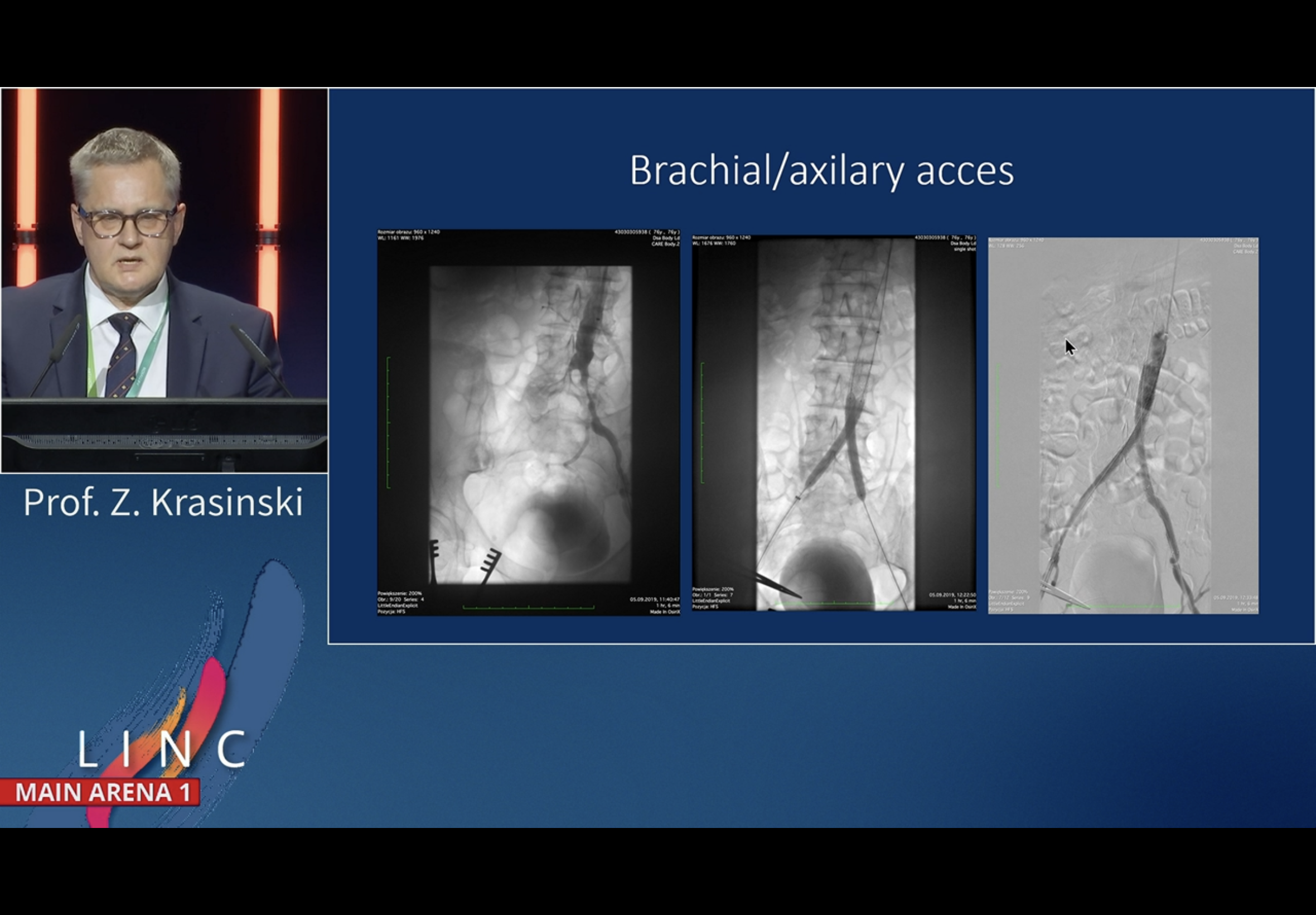
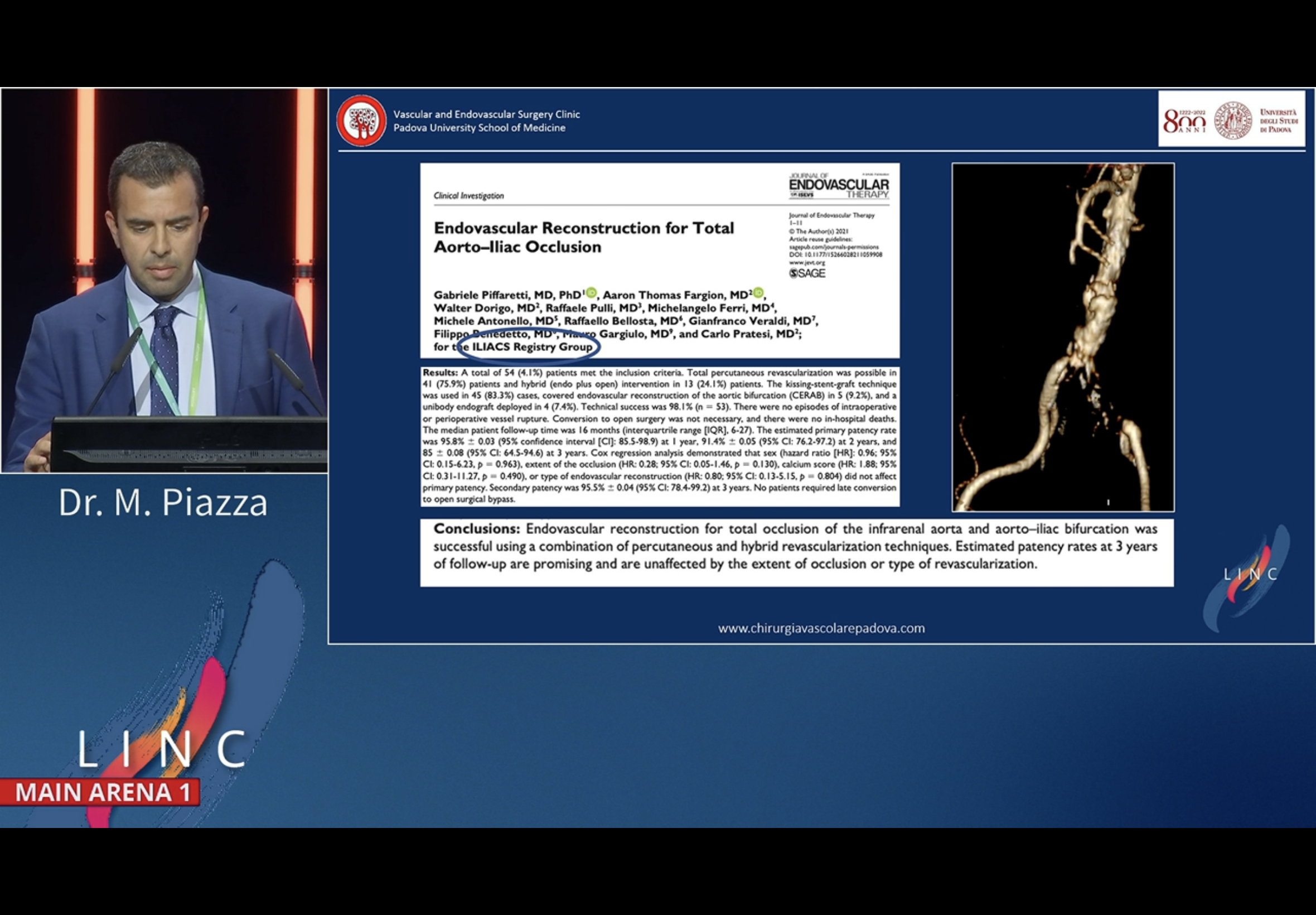
Multicentre Polish AIOD data
From Poznan
DM and CKD in about 20-25% cases
Used brachial access in only 20% patients

















BELSTREAM - first data set on BD Lifestream
Data on use of BD’s Balloon Expandable Covered stents - Lifestream - for AIOD











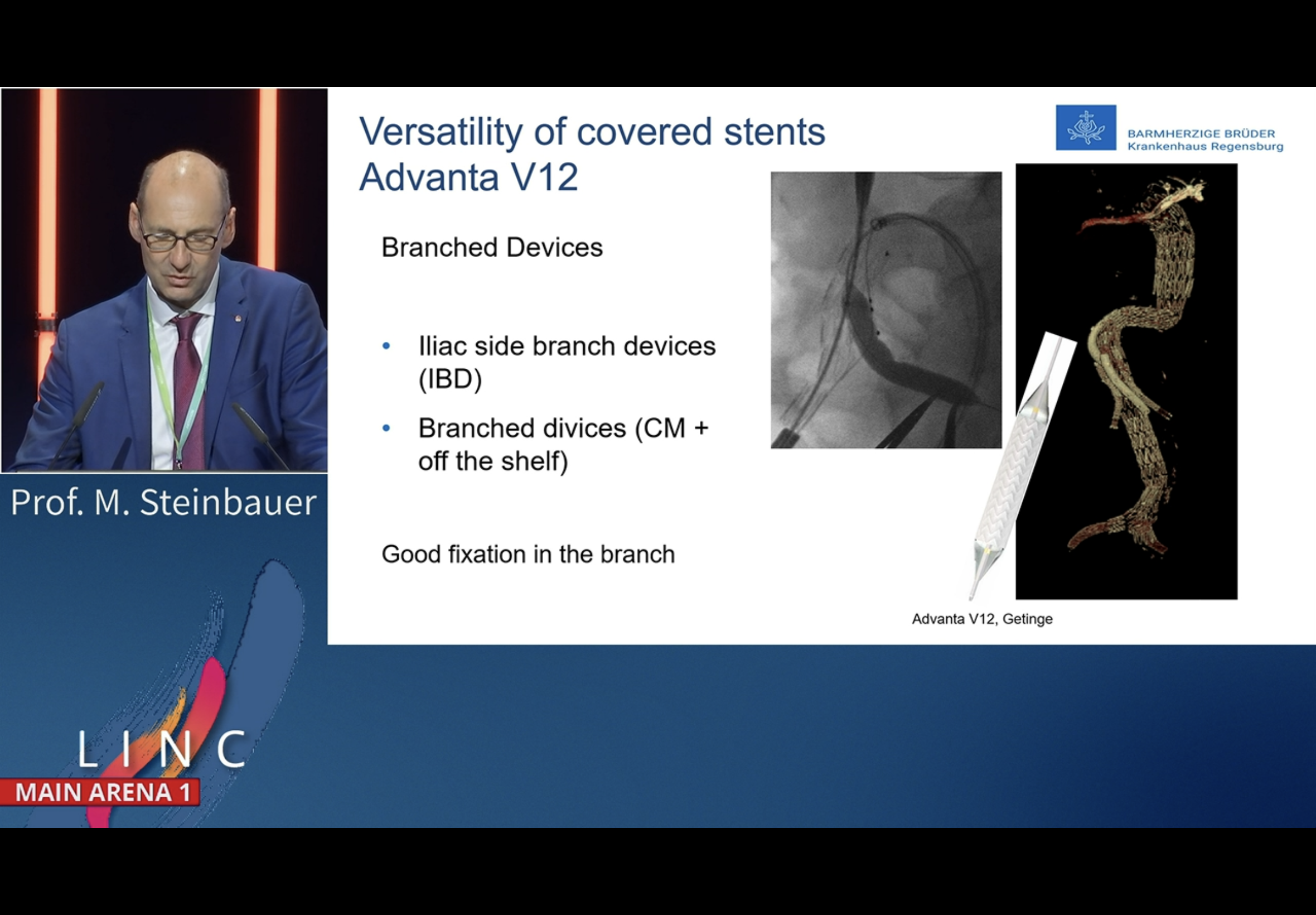










AIOD presentations on VBX and Viabahn
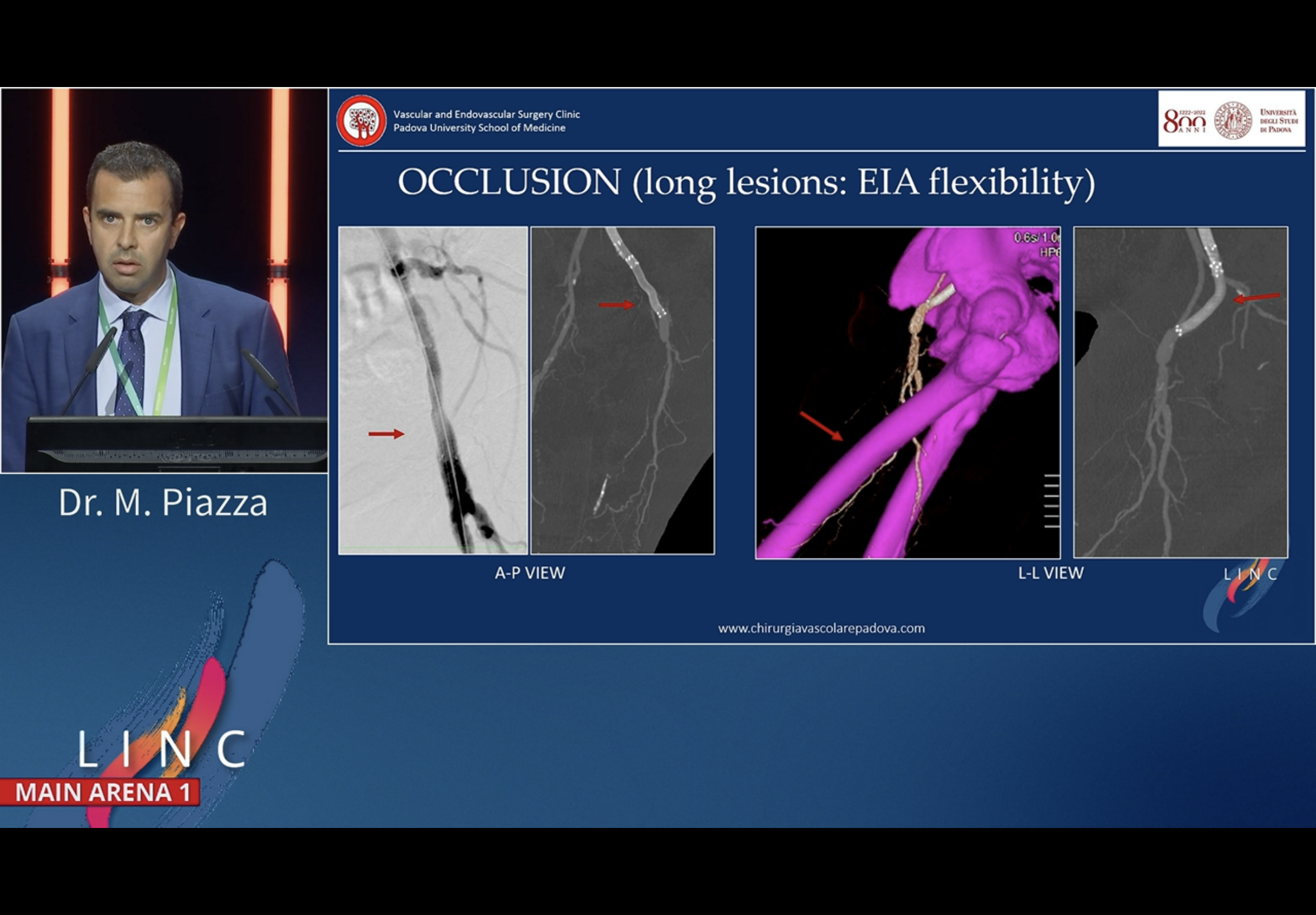
VBX slides by Jean Bismuth, Viabahn pxn by Piazza











PIAZZA - self expanding pitch











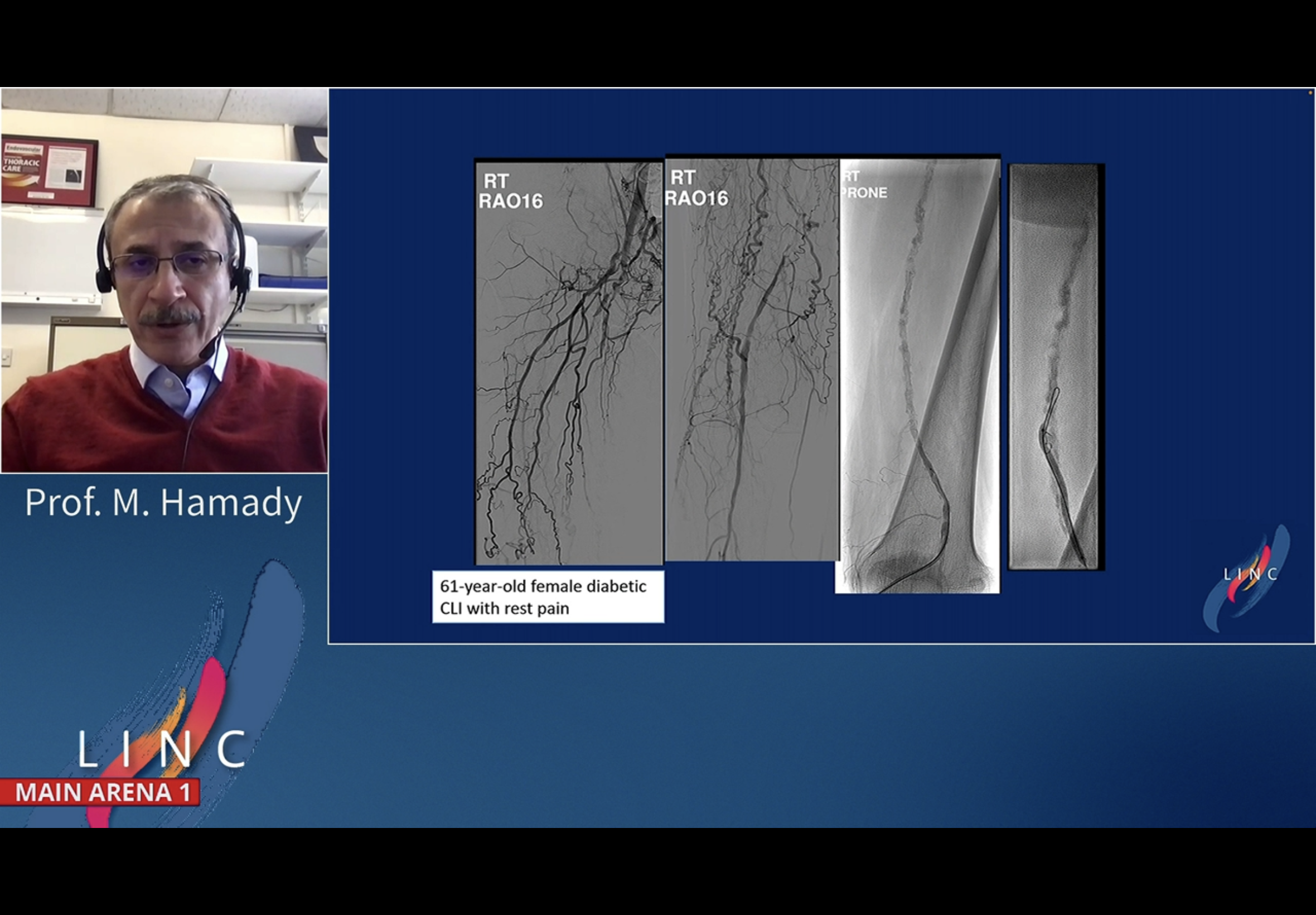
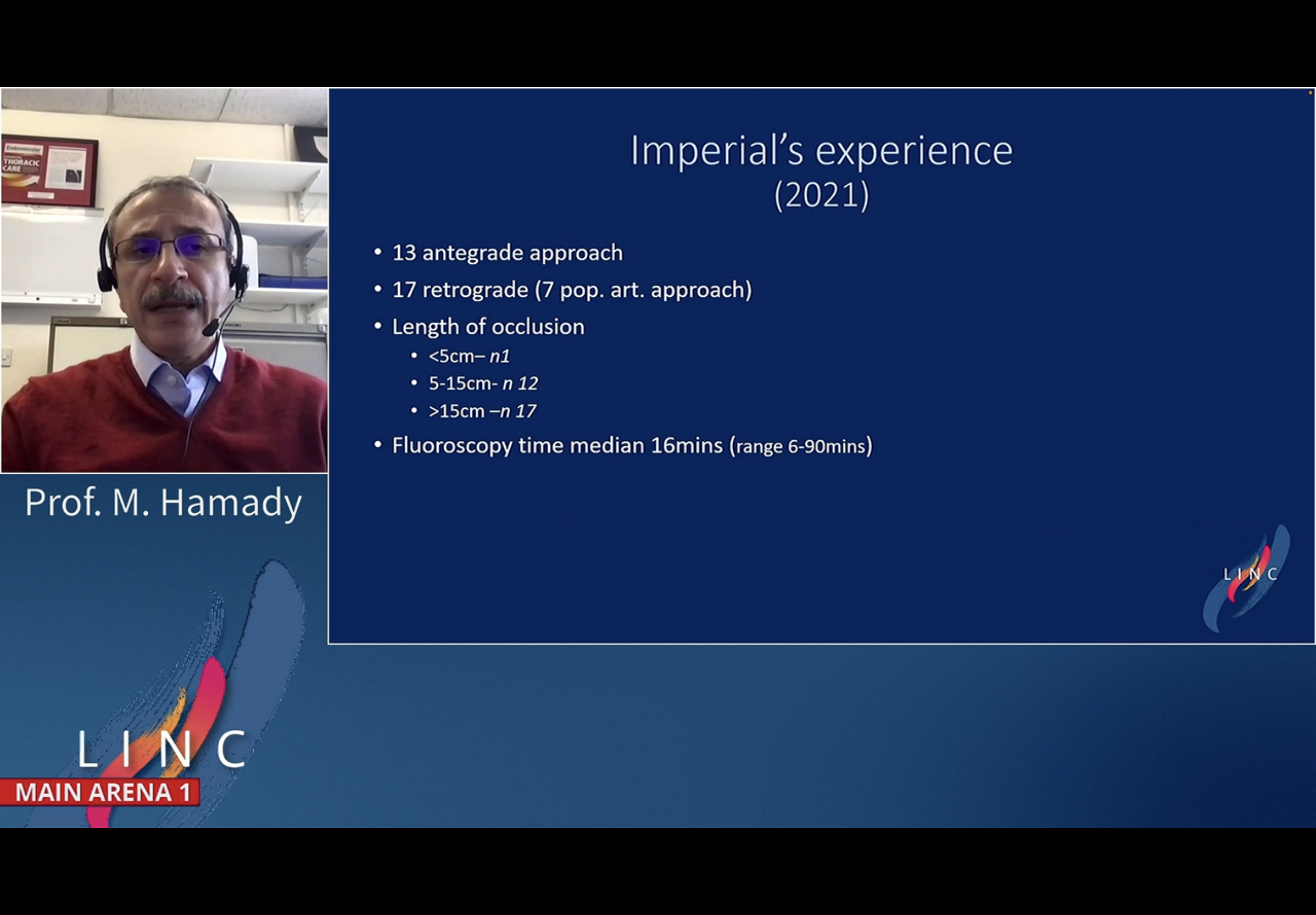
RE-ENTRY. Pioneer. Mo Hamady.
Mo Hamady from Imperial. 31 cases with a mean lesion length of 14 cm and FU of 12 months.






CERAB. Andrej. Live. 6.6.22




Commenced session with intro by Dierk Scheinert
AIOD. 6 Jun 2022 Monday is BH in Germany.
10-14 measurement on the disal aorta
not really calcified
choosing CERAB
coming from arm
Rretro up from left with Command 18 was very easy
6 balllon coming in
5F from the arm. Took a straight stiff Terumo and hammered with n o success
cut off the Judkins tip for better grip - no luck
changed to 6F at the arm and used a Multi 6F and a Judkins
Tried a CTO wire no luck
Supracore wires
somtehing about trying to get into a balloon …
different angulations to see distance between wires
Ballooned balloon below then sent the wire from above down - it passed down then into the EIA easily
useing a Jukdins wide catehter and passed the brachial wire into it - usually easy in a narrow EIA
Now chaning from 18 to 35 system for better stability
Now - decide “what to take in”



















REturn3ed to Andrej after 4 talks, case completed. Has placed a large single aortic stent and then CERAB reconstructions from both groins. Interestingly did not have retained wire cacess from teh left recanalised CTO while he deployed the top aortic!
Used V12s all the way through I think?















CERAB. Andrej. Live. 6.6.22 (Copy)
Commenced session with intro by Dierk Scheinert
AIOD. 6 Jun 2022 Monday is BH in Germany.
10-14 measurement on the disal aorta
not really calcified
choosing CERAB
coming from arm
Rretro up from left with Command 18 was very easy
6 balllon coming in
5F from the arm. Took a straight stiff Terumo and hammered with n o success
cut off the Judkins tip for better grip - no luck
changed to 6F at the arm and used a Multi 6F and a Judkins
Tried a CTO wire no luck
Supracore wires
somtehing about trying to get into a balloon …
different angulations to see distance between wires
Ballooned balloon below then sent the wire from above down - it passed down then into the EIA easily
useing a Jukdins wide catehter and passed the brachial wire into it - usually easy in a narrow EIA
Now chaning from 18 to 35 system for better stability
Now - decide “what to take in”
REturn3ed to Andrej after 4 talks, case completed. Has placed a large single aortic stent and then CERAB reconstructions from both groins. Interestingly did not have retained wire cacess from teh left recanalised CTO while he deployed the top aortic!
Used V12s all the way through I think?