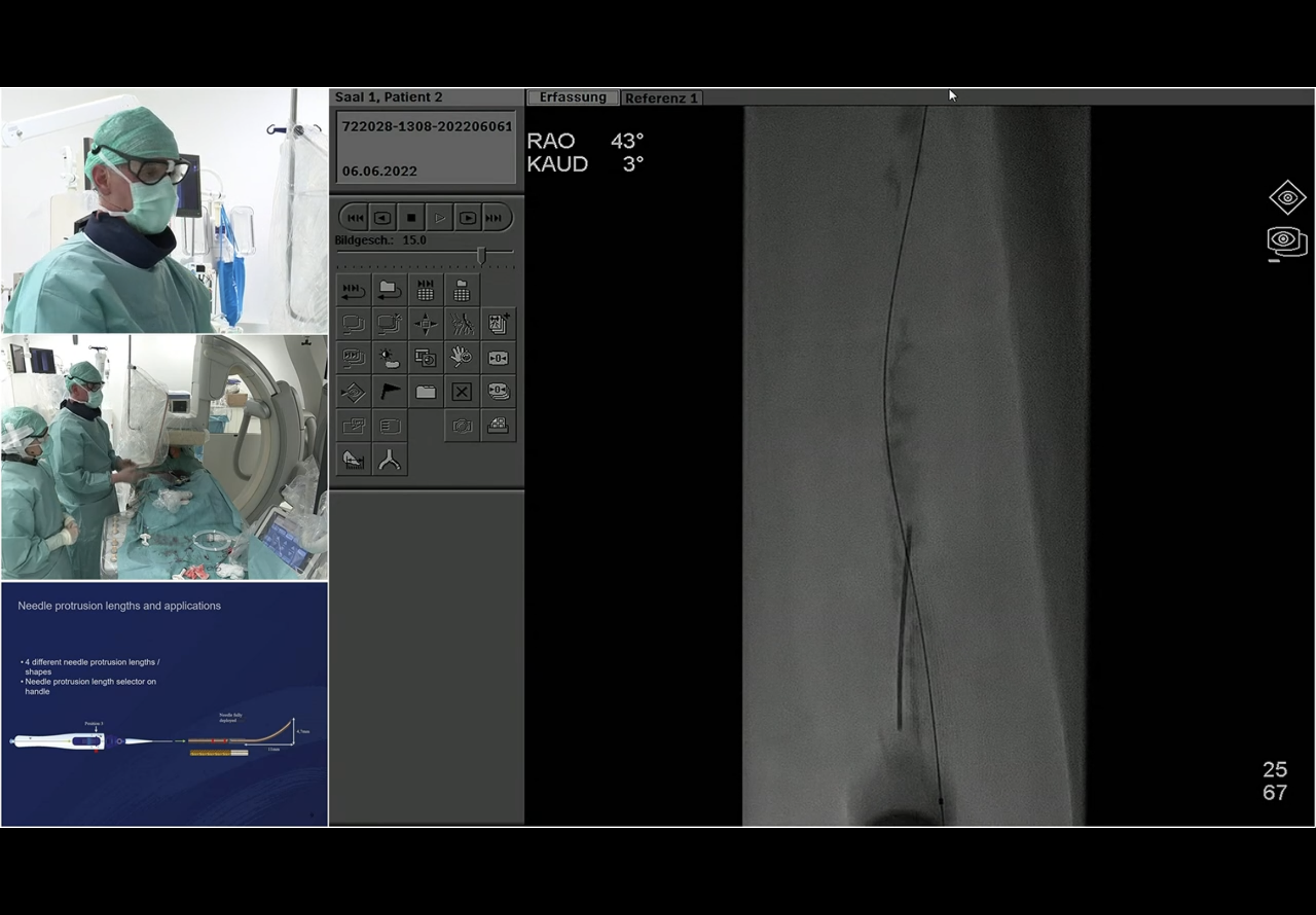
Leipzig Live case Mon 6th Jun 2022 @ 17.25h
Showing the GoBack catheter. Andrej.
Comes in 90 and 120 shaft, it is a 4F catheter.
Too much Calcium, no IL option have to go around the calcium.
Andrej has shoved a lot of LA into the calcium.
Predilated with 3mm balloon.
Then an ultra score 5x200.
after the break
used a high pressure 6 x 40 conquest at 40 ATM
Got a bleed in the adductor.
No pain
Using a 7.x 40 balloon
Lots of bleeds
Used a Viabahn therefore - 7 x 150
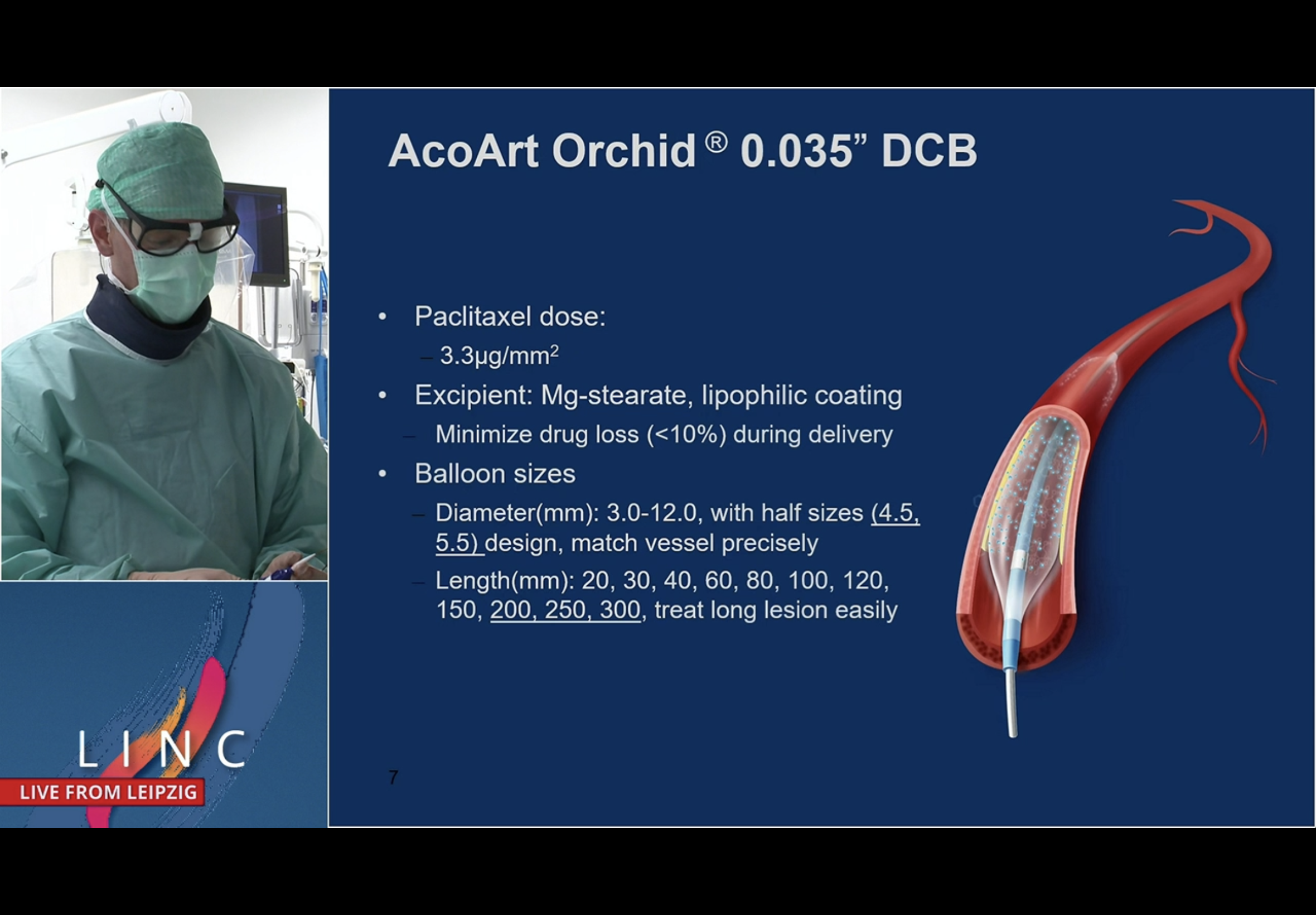
Orchid 6 x 120 DCB distally
Proxammly also DCB
He will still use a Supera because of the late recoil concern (so will place it INTO the Viabahn)
































































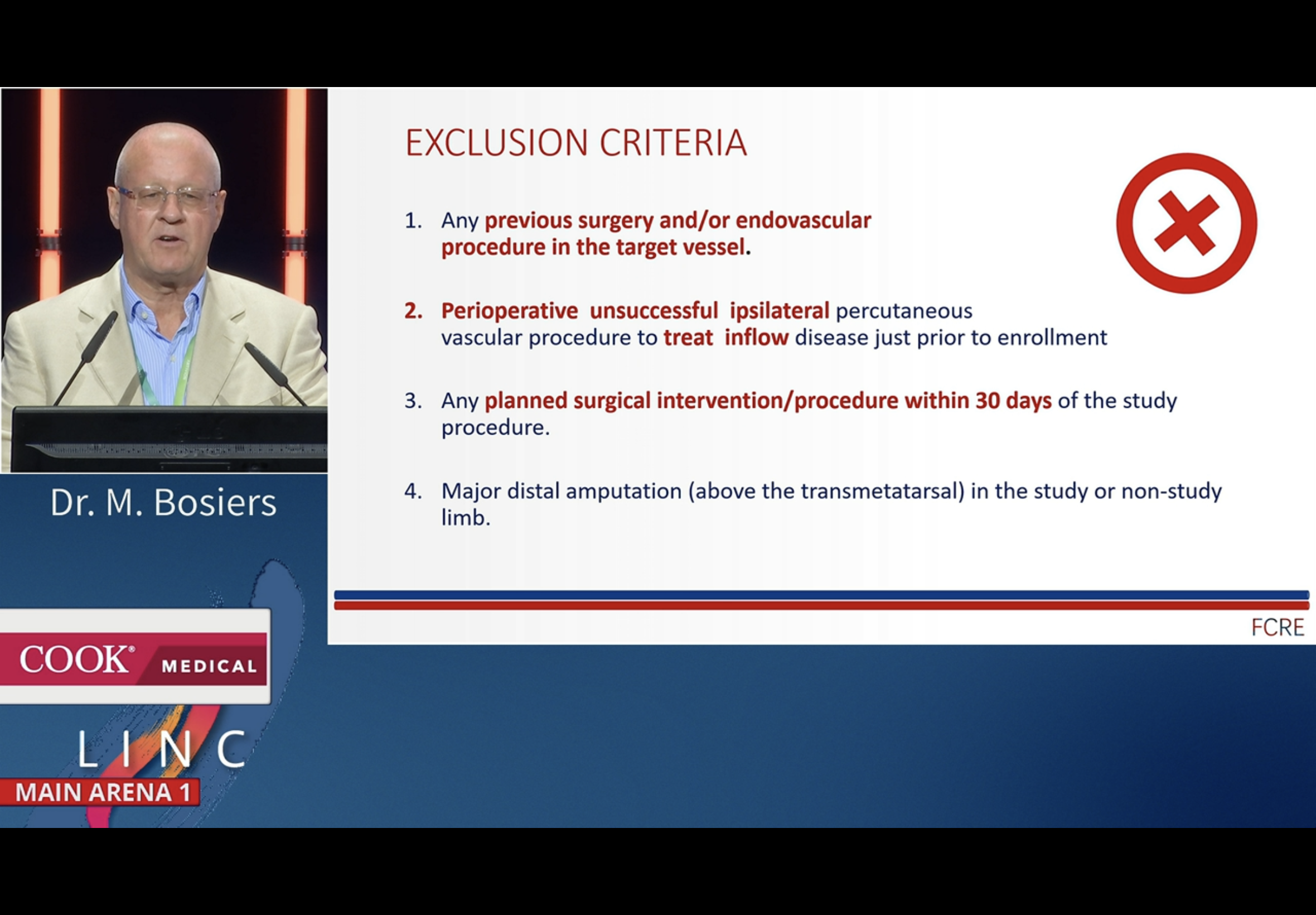
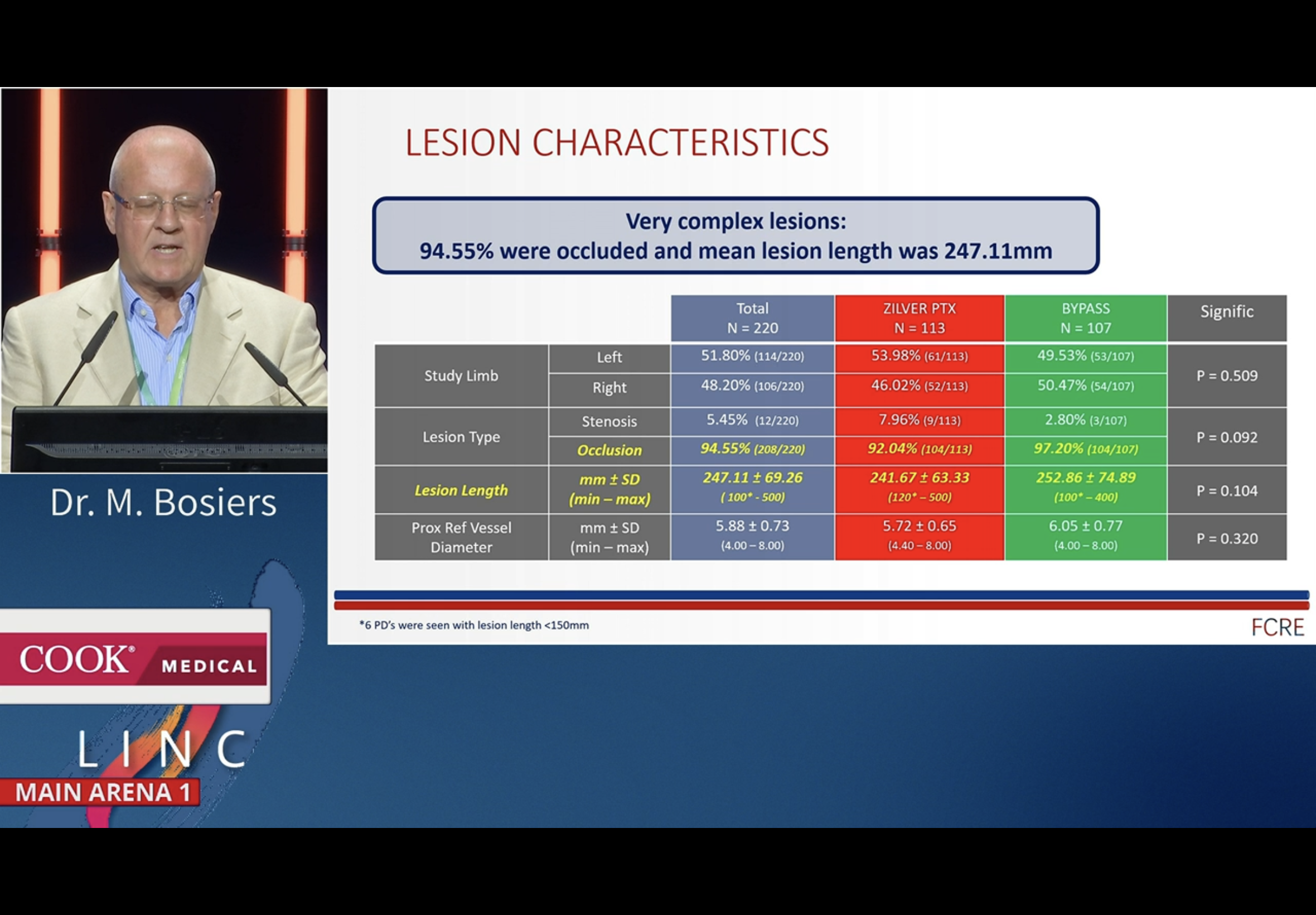
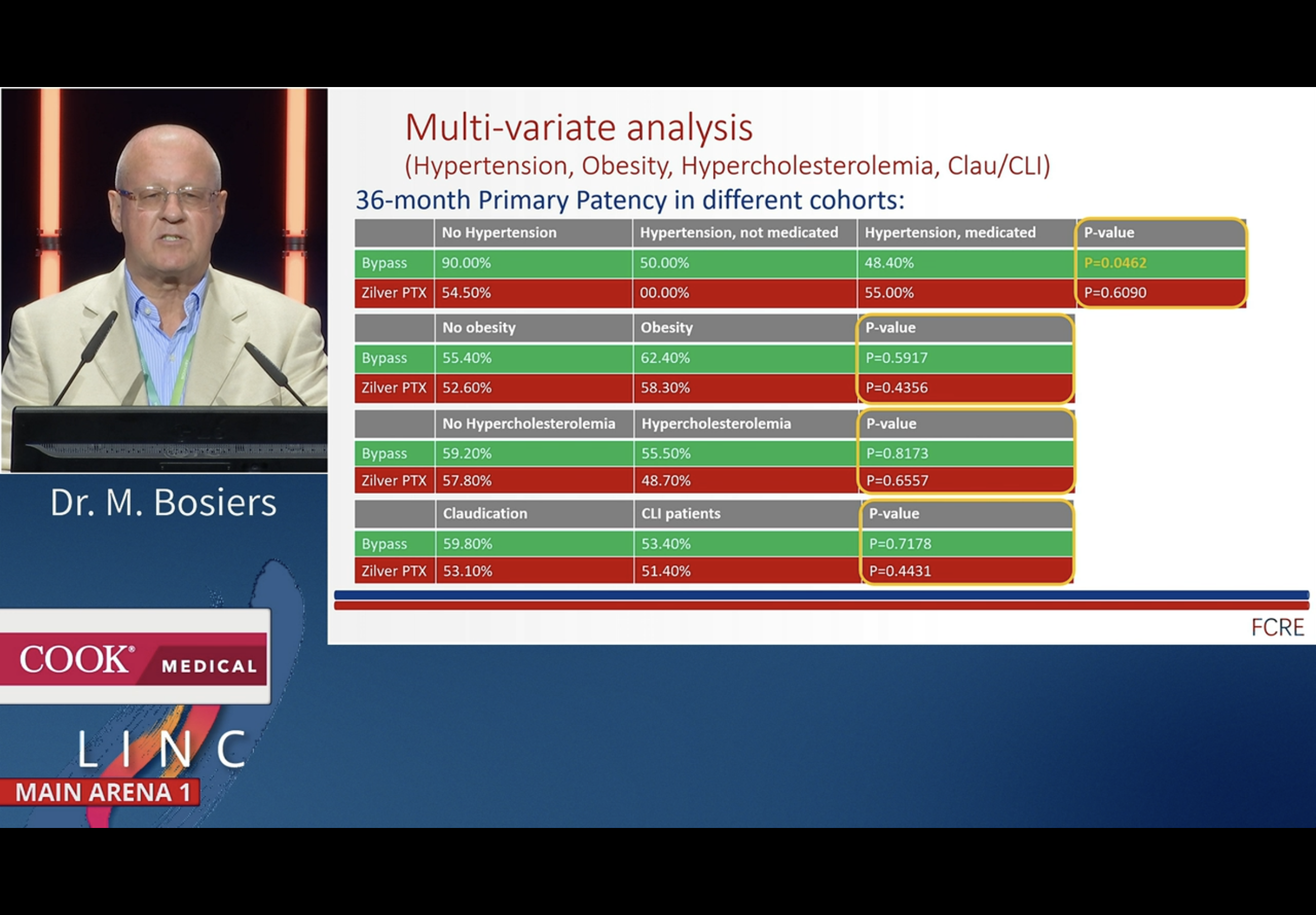
Zilverpass - 36 month update
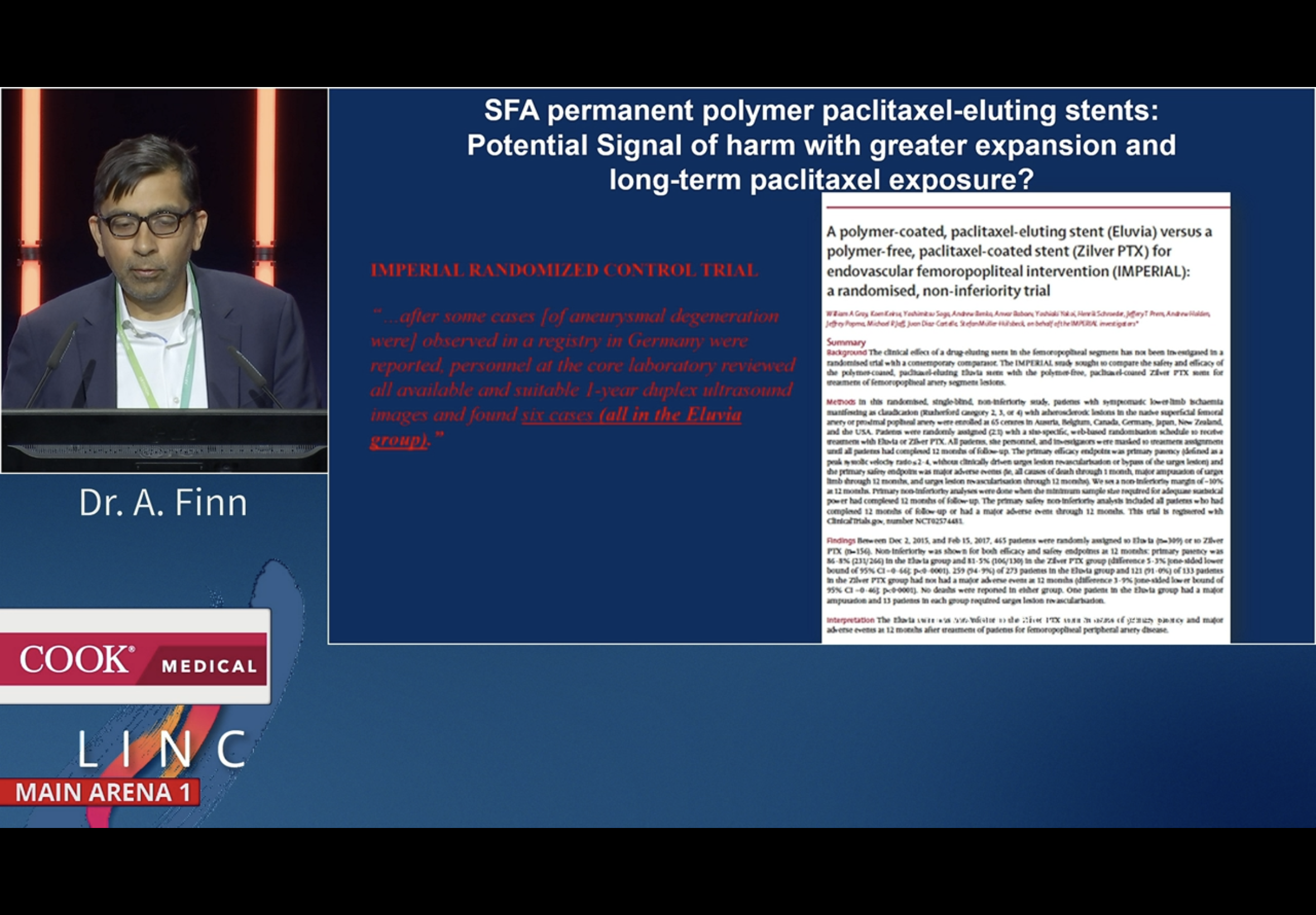
2020 Zilver PTX Pacli stent v FPBG non inferiority outcomes safety and efficacy












Polymer coated DES - multiple talks
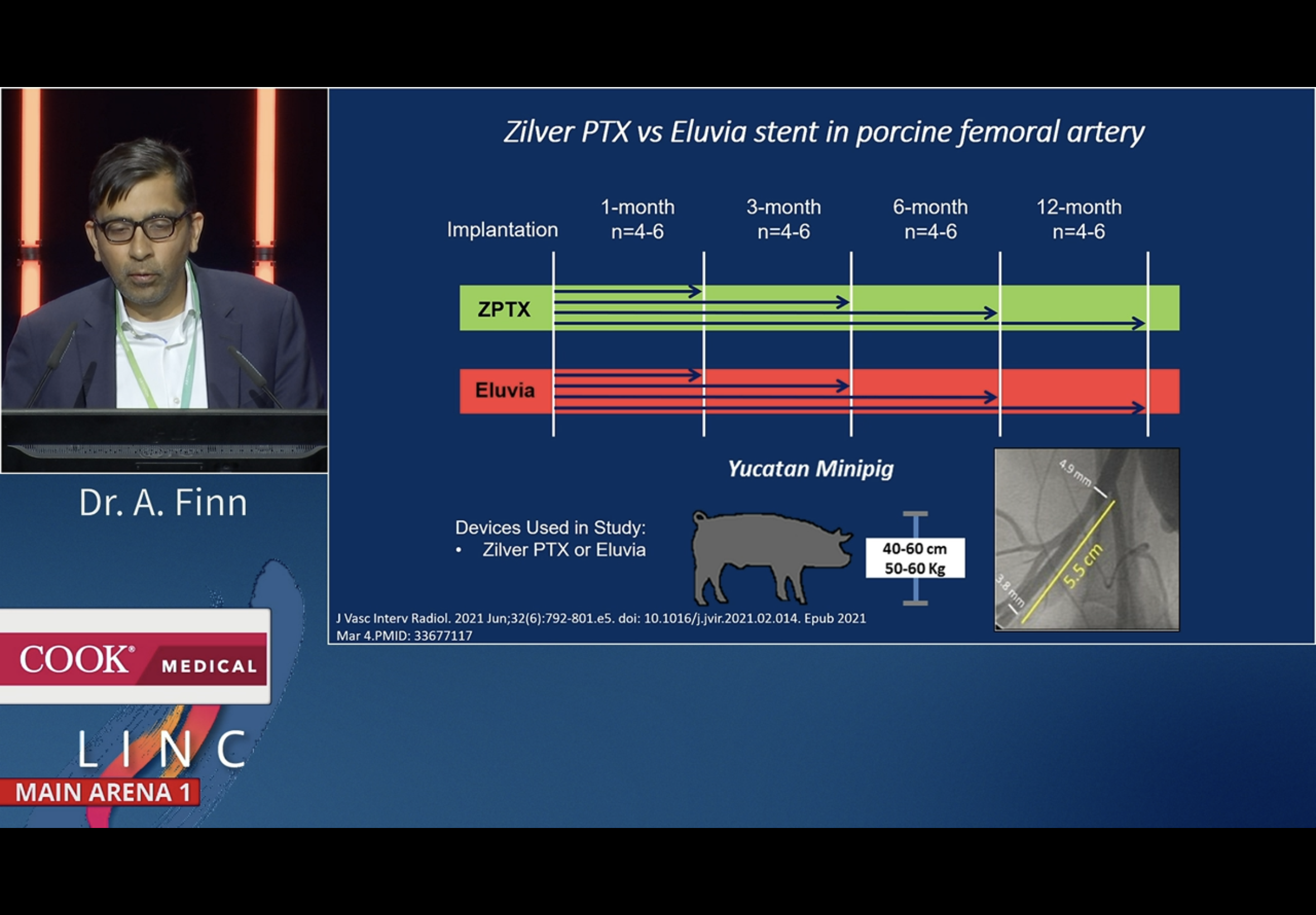
Aloke Finn preclinical research.
good comparison of the polymer Eluvia low dose and polymer free higher dose Silver PTX
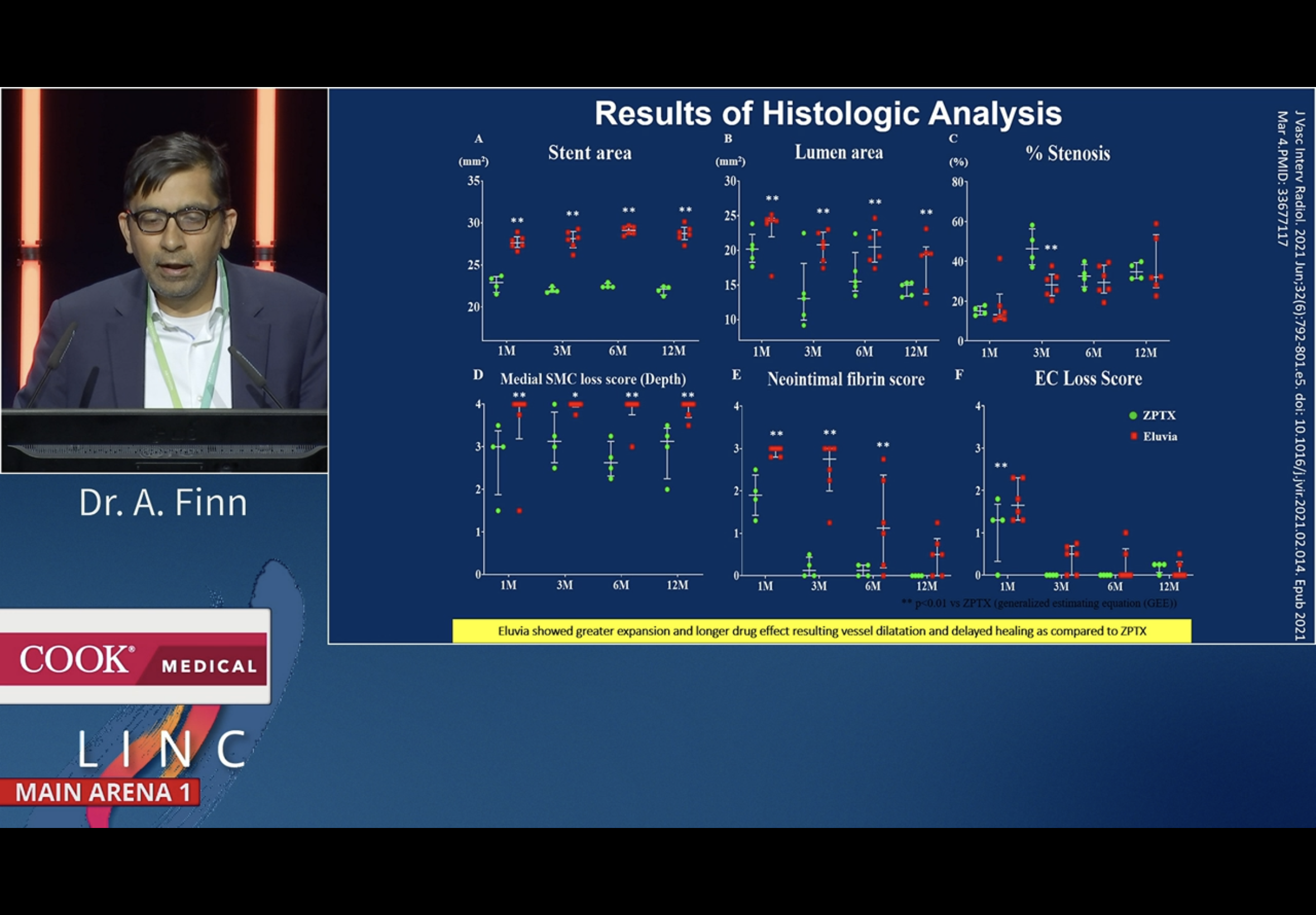
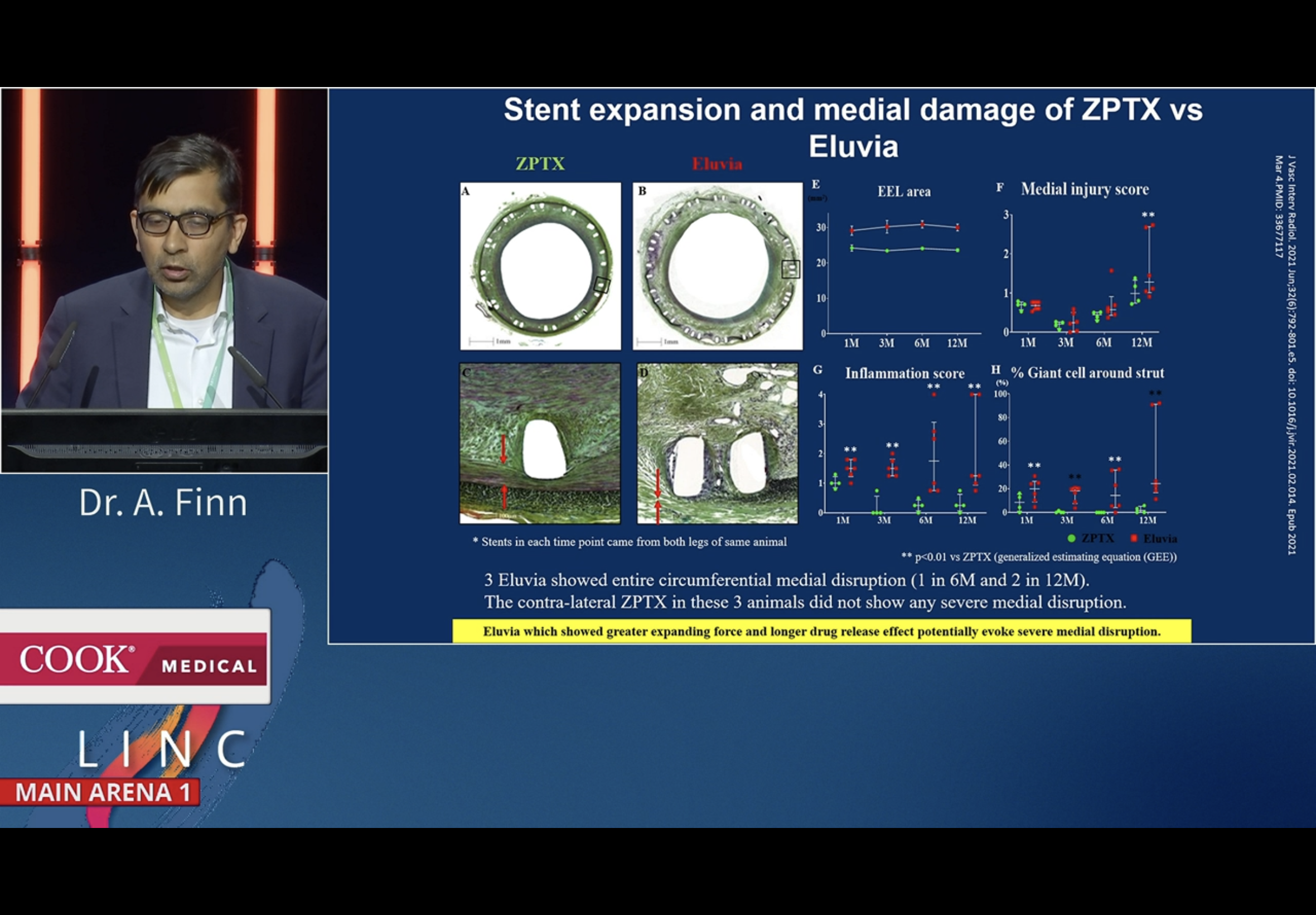
Higher dose Pacli reduces hyperplasia but does also slow down healing
much less medial SMC loss on Zilver
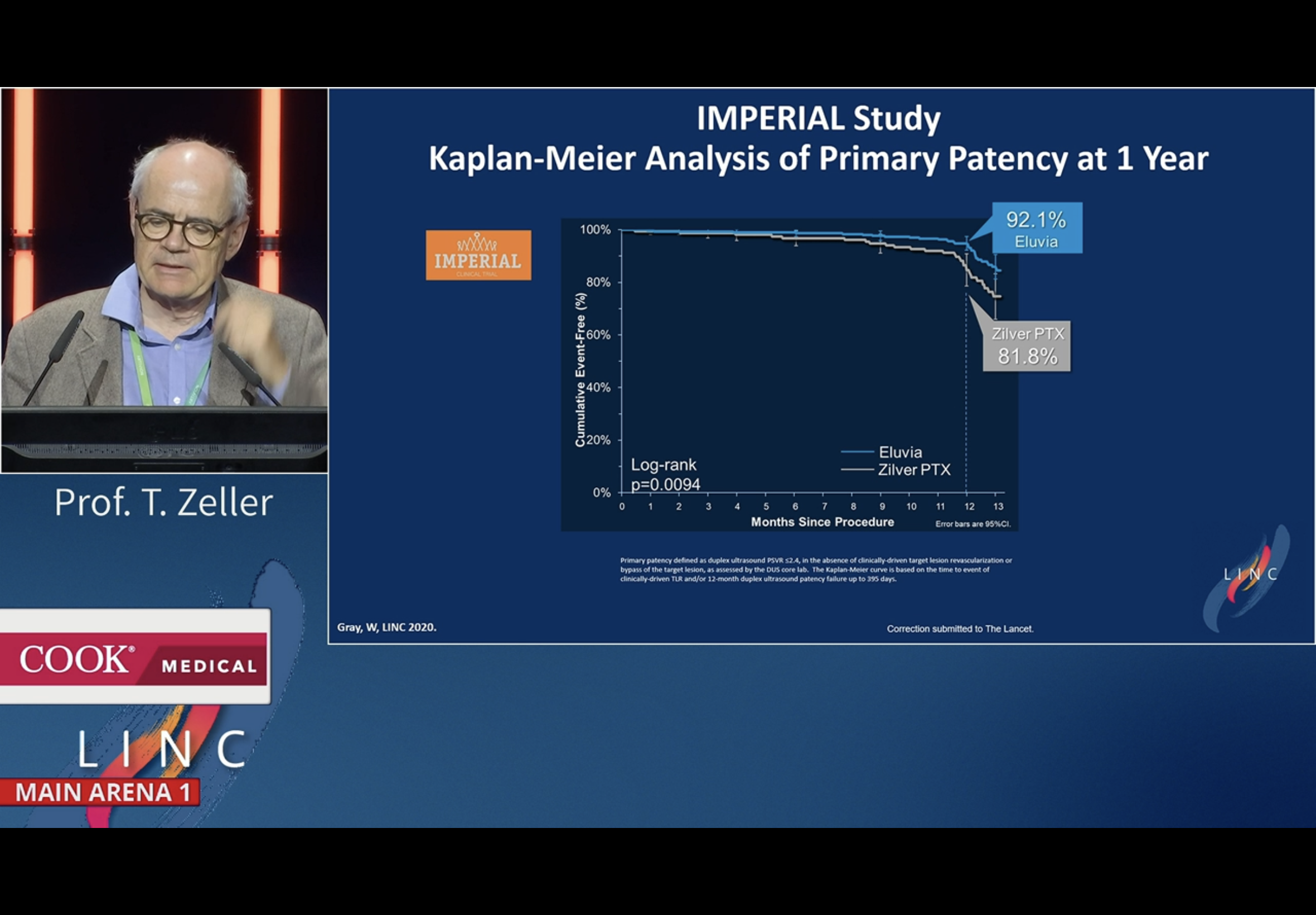
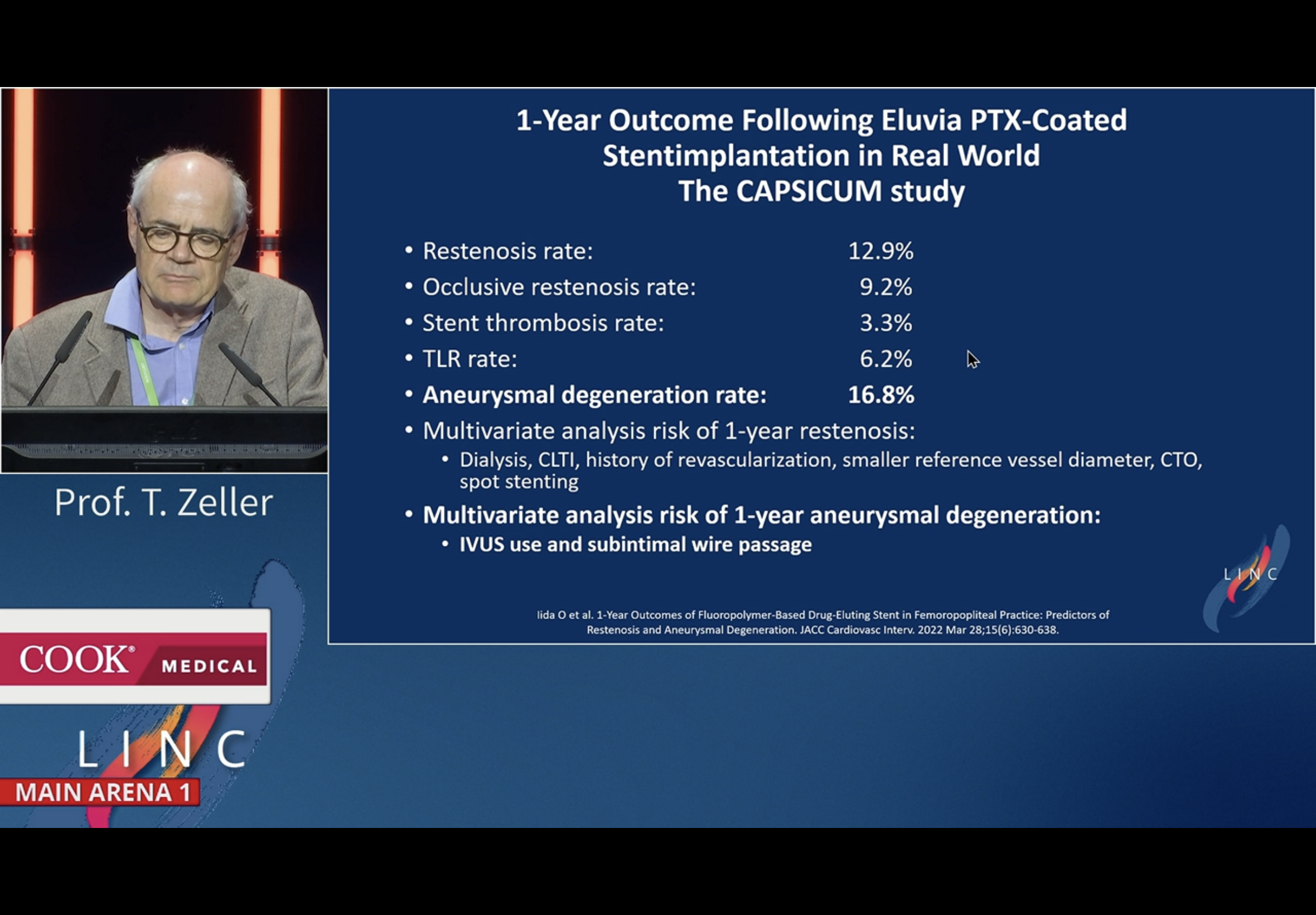
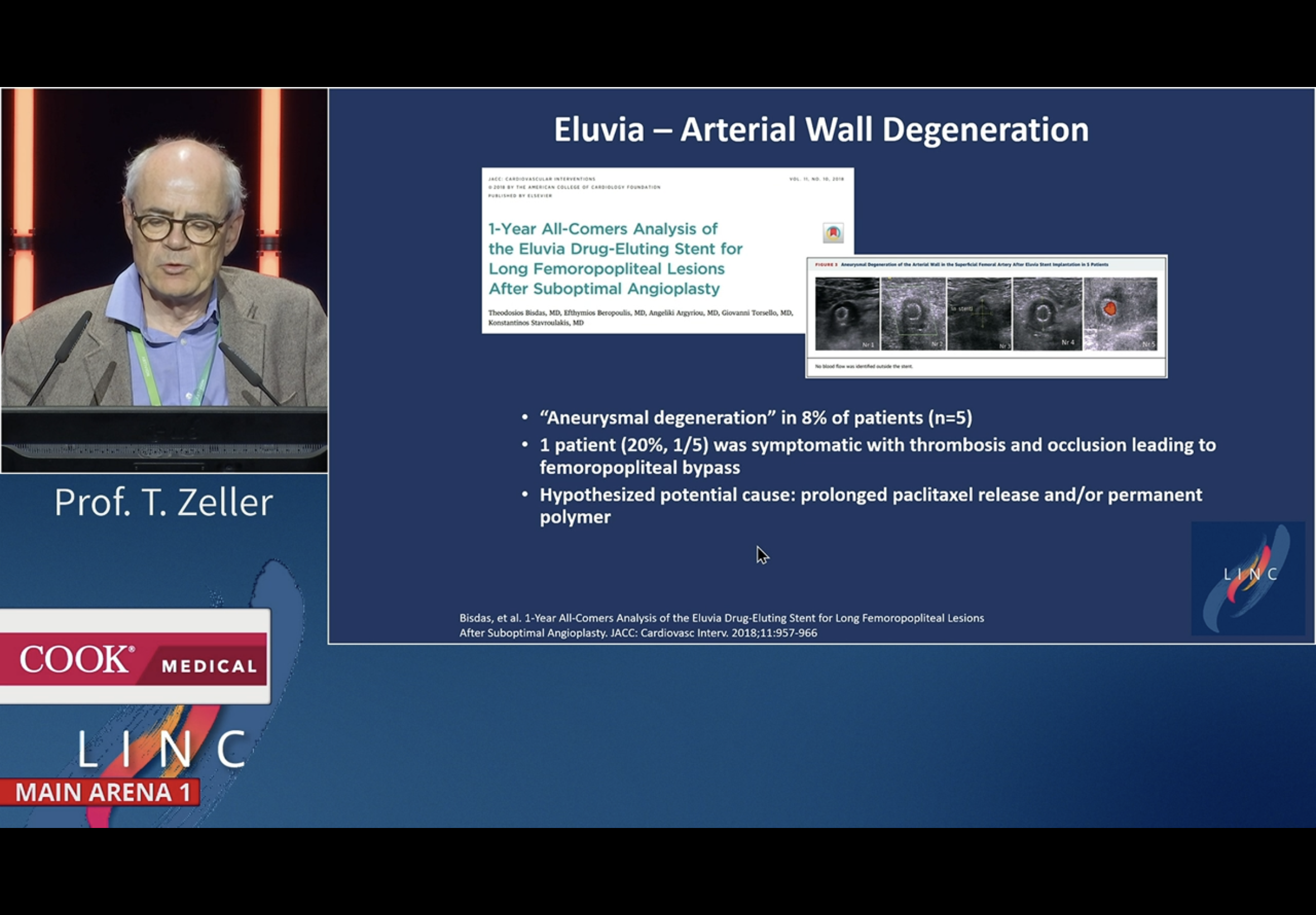
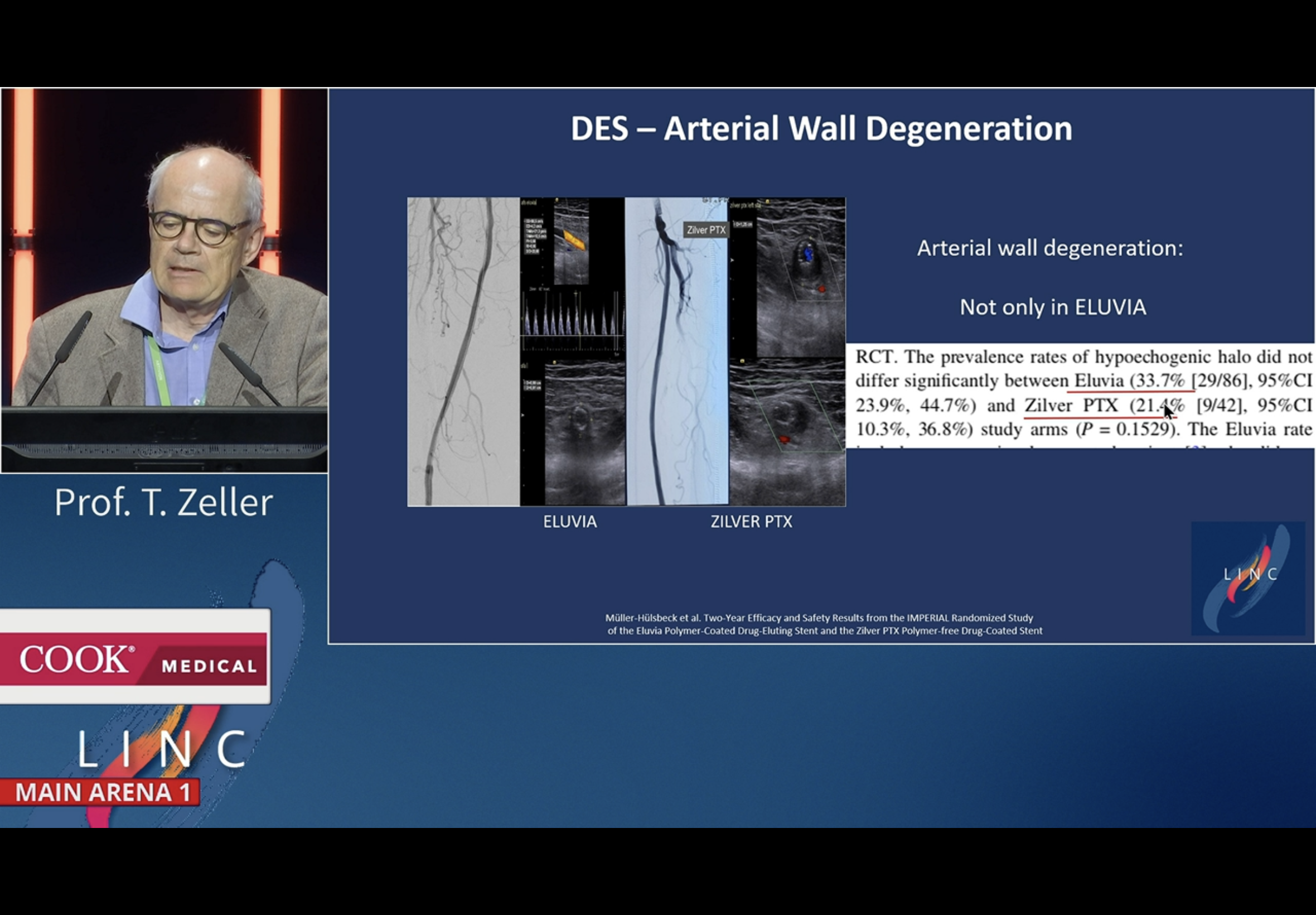
Next talk : Clinical comparison of the stents by Thomas Zeller
Much made of the halo sign and guidance for surveillance offered by TZ.
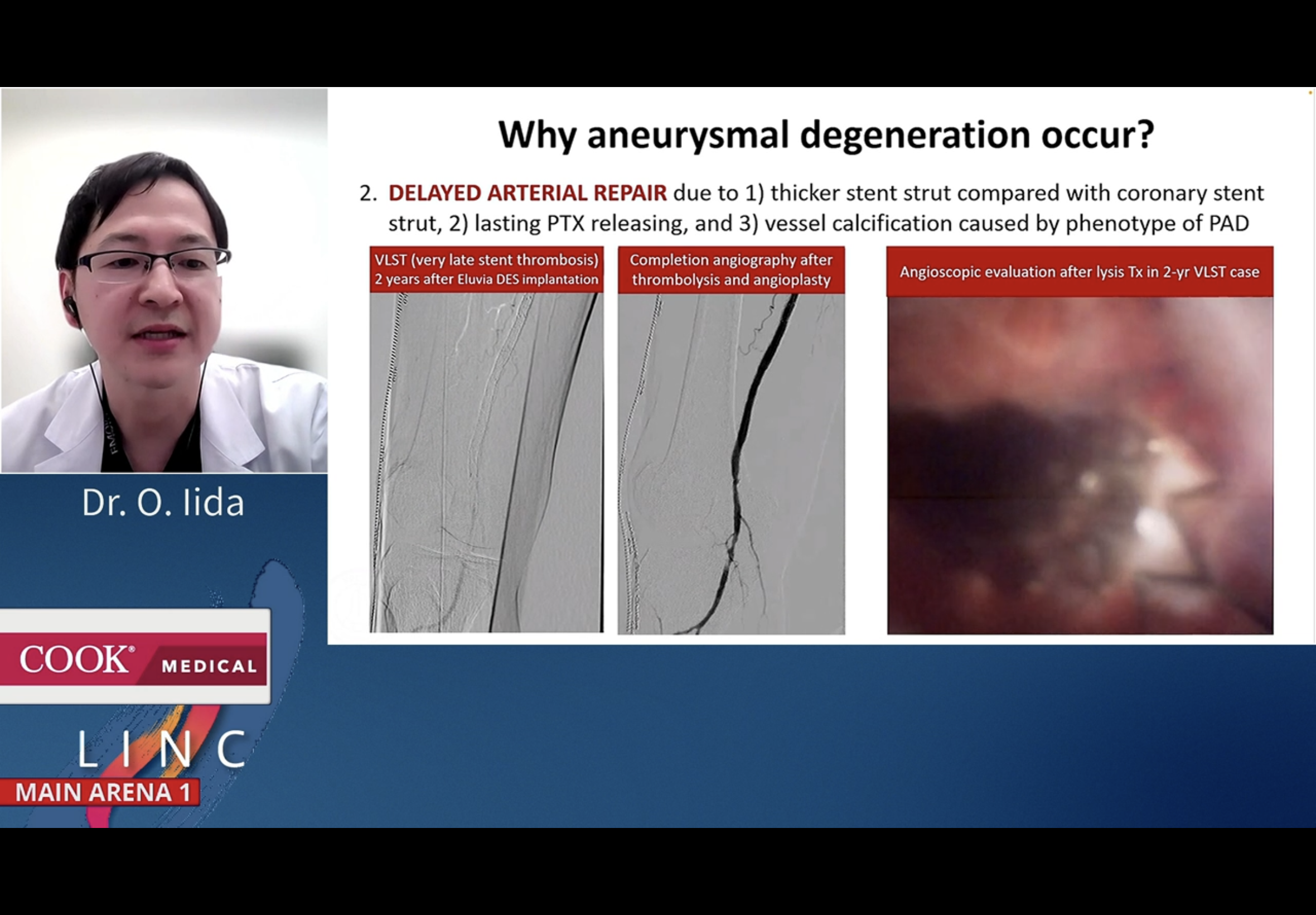
Osamu Lida. Angiography and IVUS. Case study analysis.
Questions from Deloose. What do we name this problem? Delayed arterial repair? Vessel enlargement? Aneurysmal change? Inflammatory halo sign?
Zeller: not known if clinically relevant. certainly not that frequent to find enragement with flow (as opposed to the non flow halo). homogenous area around the stent is probably infmallation and not significant, and also seen with bare metal stent. Actual aneurysmal change is different matter.
Aloke Finn. Agrees that there probably are 2 different manifestations. Struts elute the drug - the destruction is around the struts.
Marc Bosiers: yes need to differentiate from intraluminal and extraluminal. Should FU pts closely - at least every 6 months with duplex.
Marc Bosiers: learn from cardiologists. They look with ICT or IVUS pre and post Rx at the vessel wall.
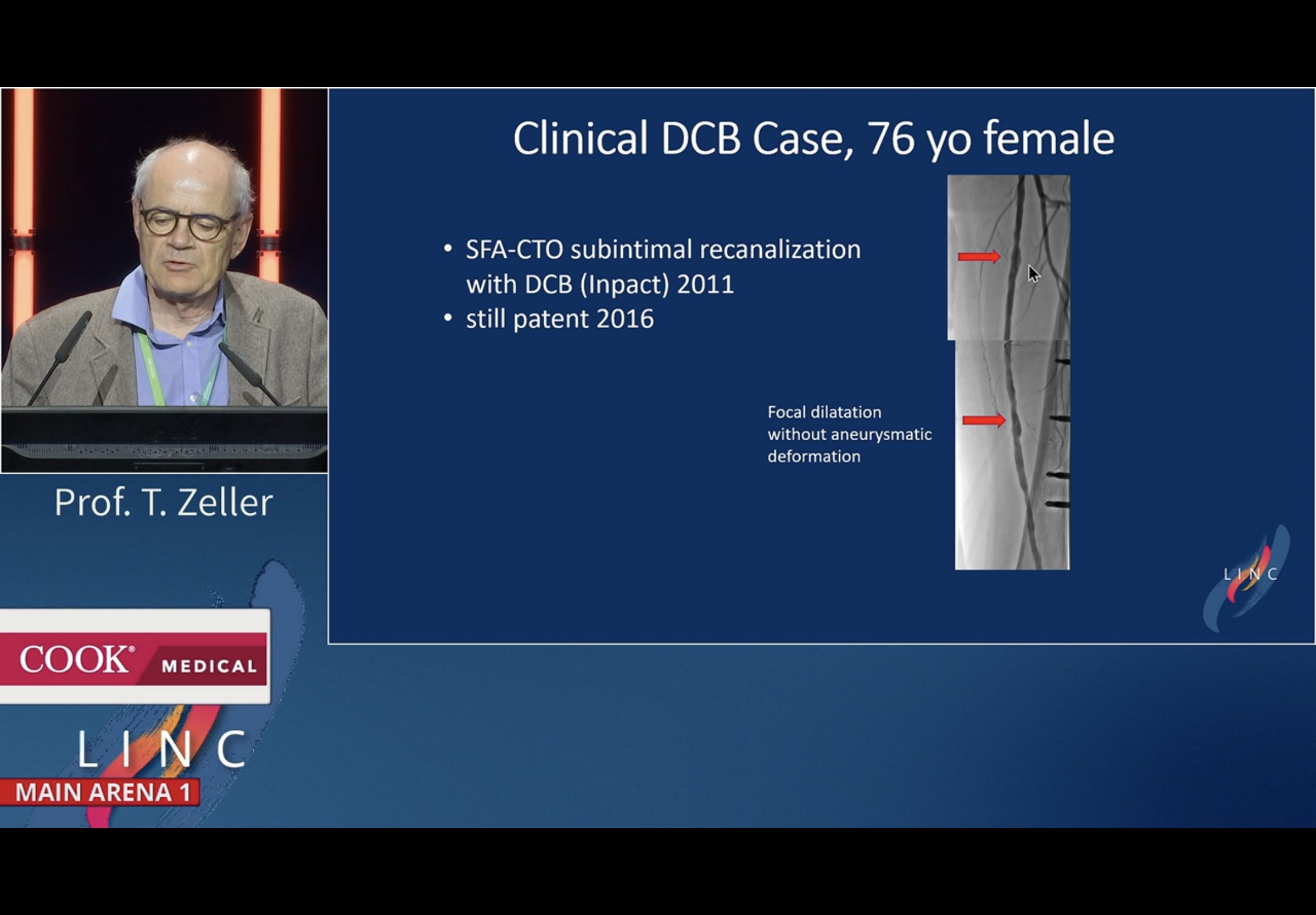
Deloose: What is the position regarding all this with respect to DCB?
Zeller: need to be extra careful when doing subintimal. If a big subintimal loop perhaps need to entirely avoid any drug…
Aloke: Big difference between a DCB and a polymer coated stent. But agree with TZ re the vessel wall damage.
Debus: stating example of endarterectomy - feels not quite the media loss or vessel damage that is relevant but the drug (Paclitaxel) as it is toxic.










































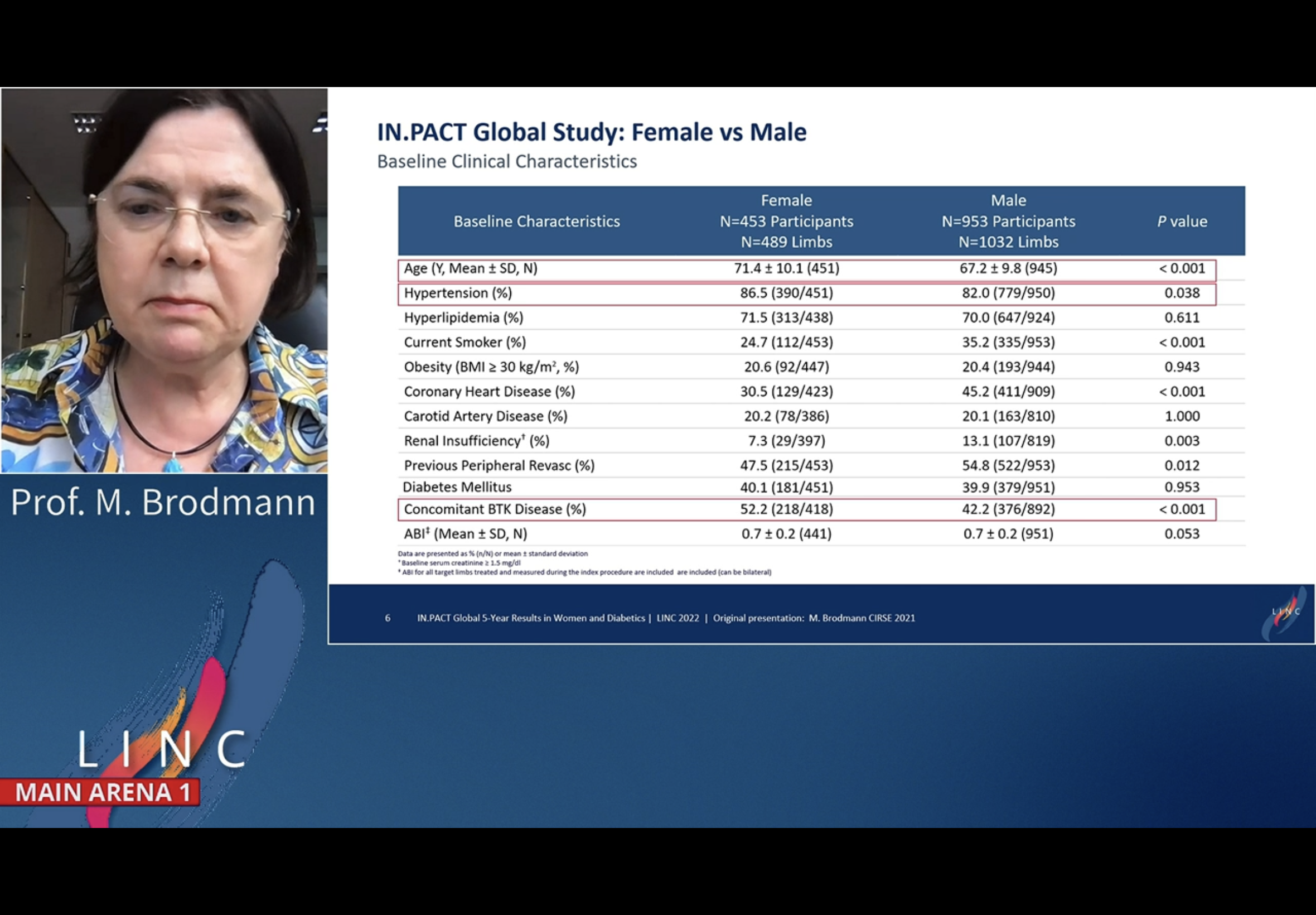
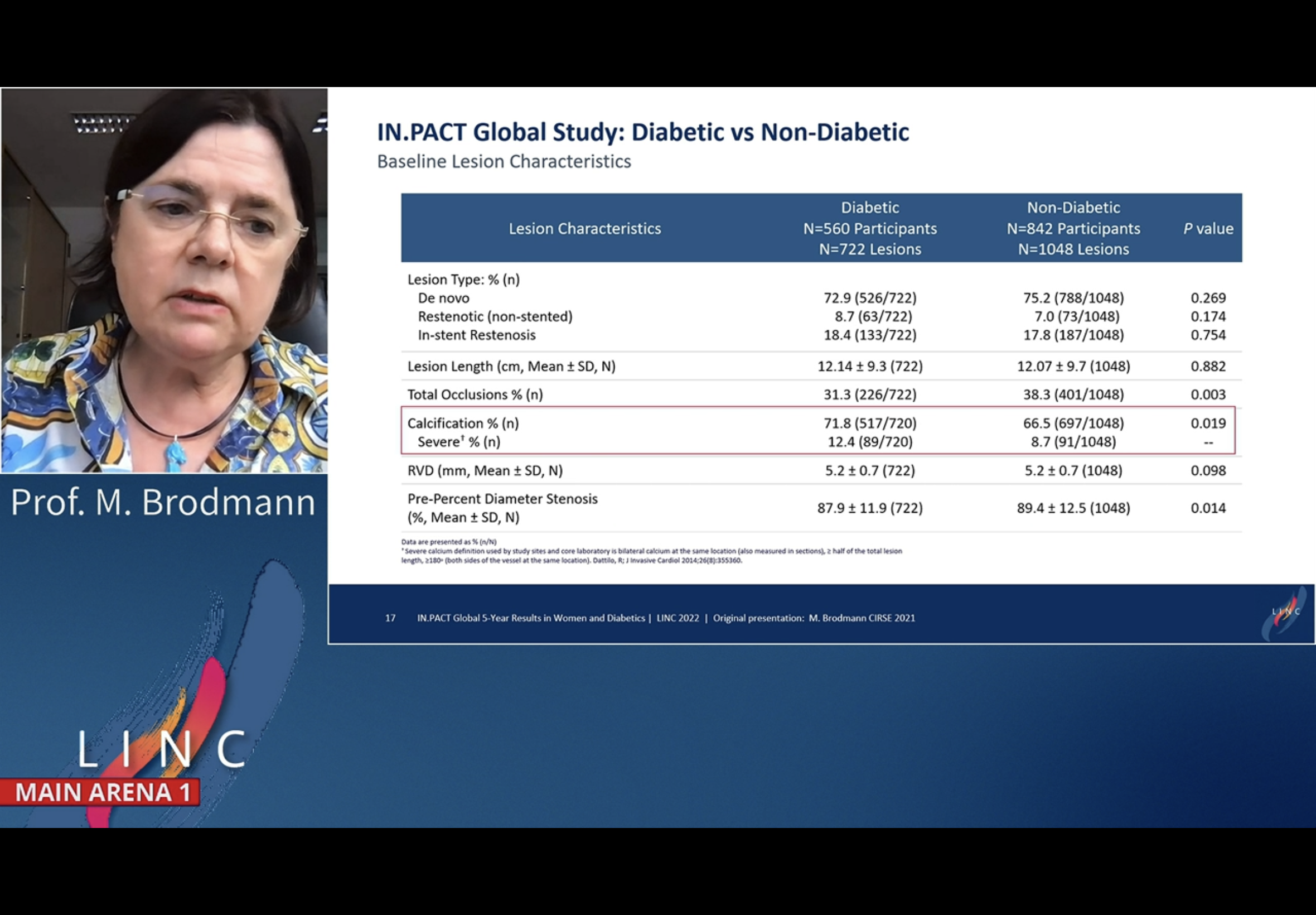
IN.PACT subgroups (DM and gender) - Brodmann
A different DM talk first
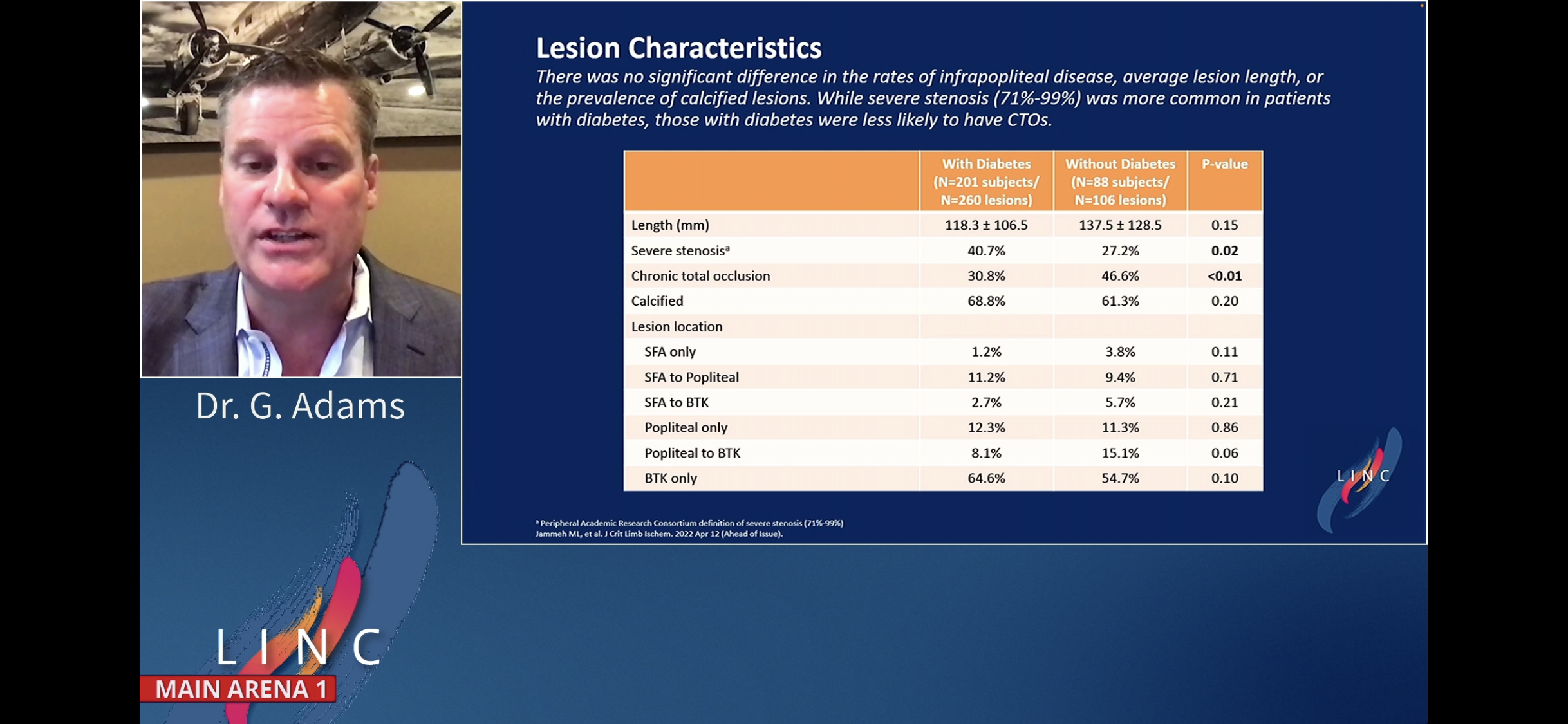
LIBERTY
George Adams NC USA





















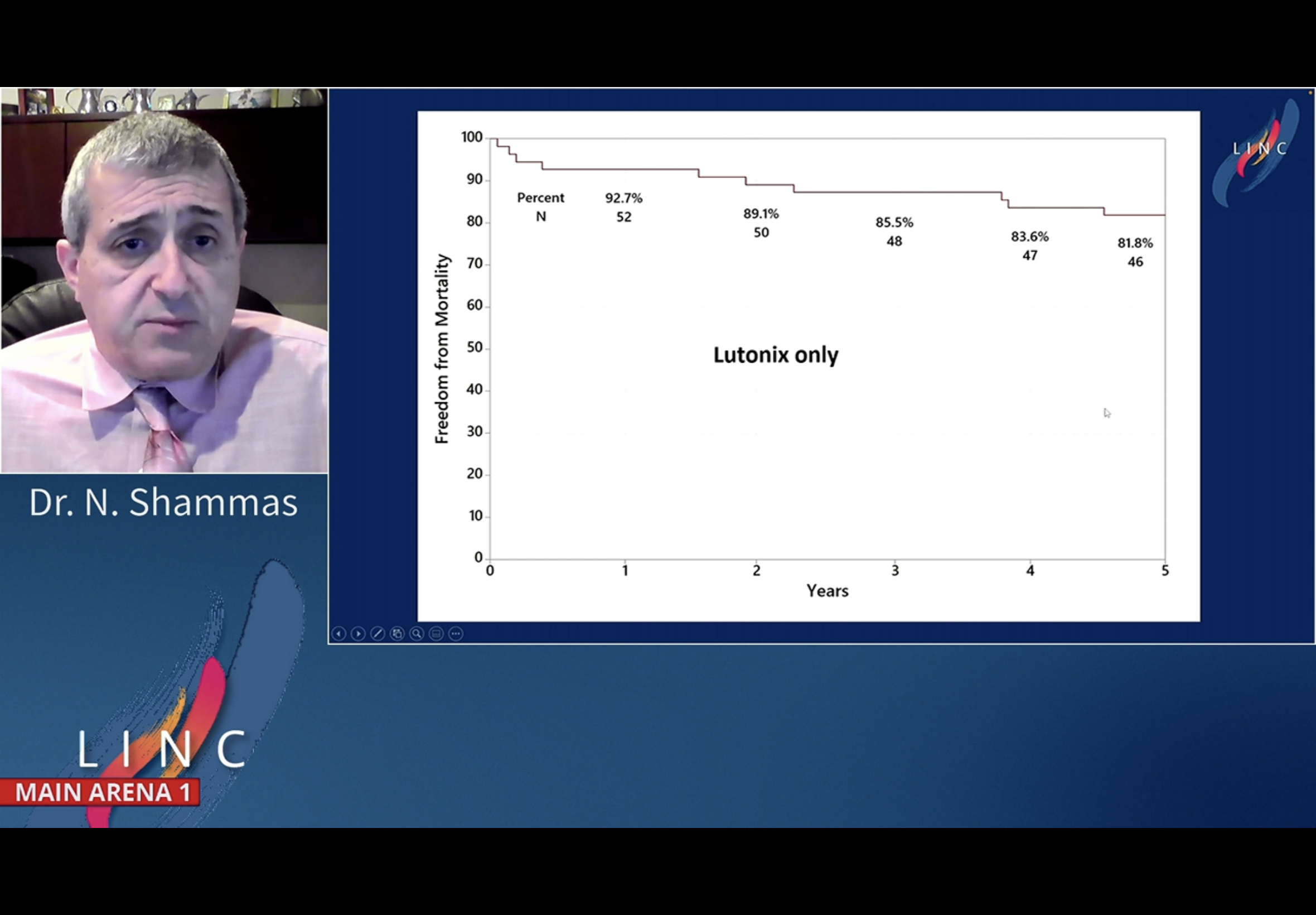
Lutonix trial 5y results - Shammas
First 5 year data any DCB
Evaluated in response to Katsanos
Analysis of treated segment length v. mortality














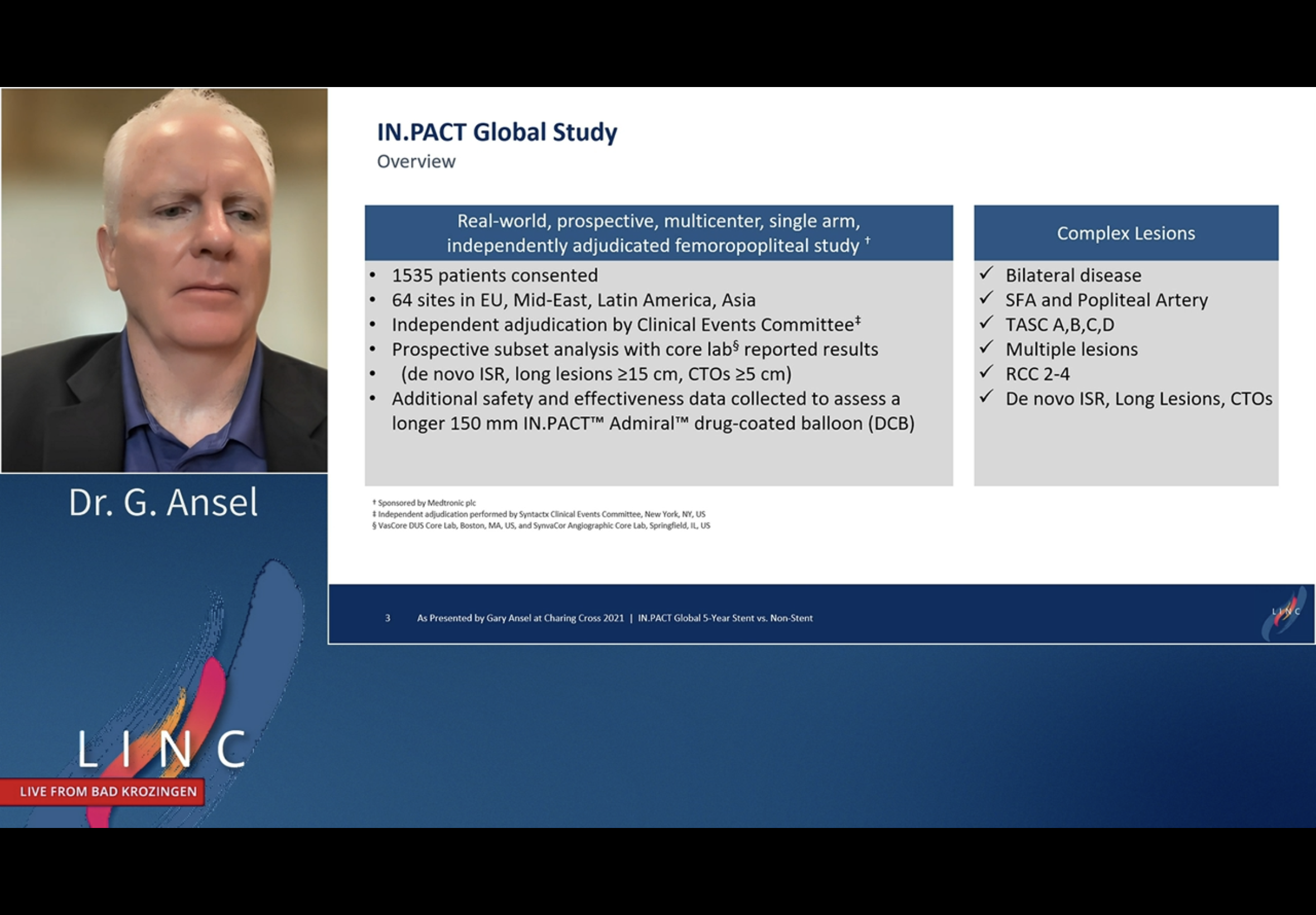
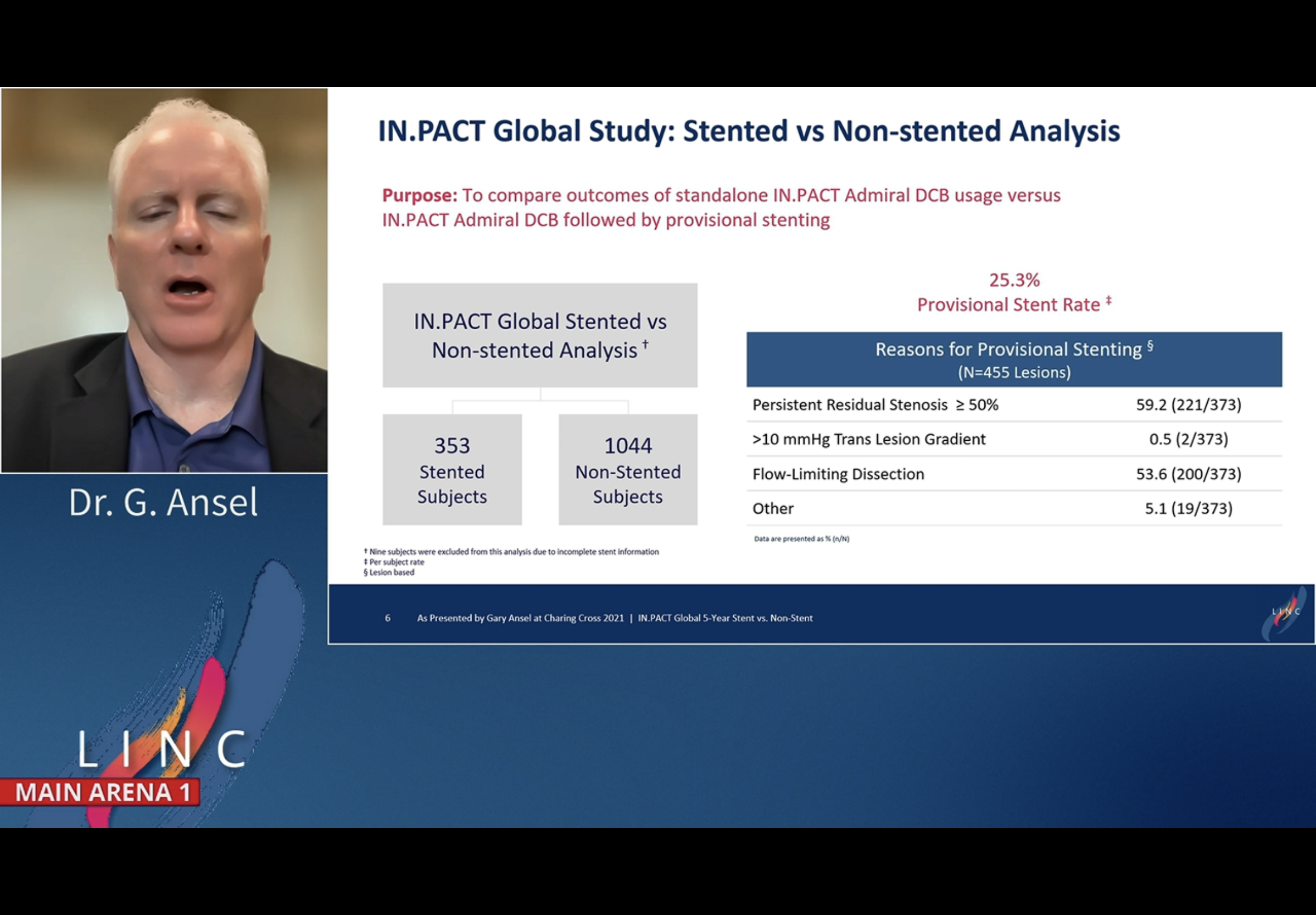
DCB v DCB+stent IN.PACT 5 year data
Women were older, more CVS disease and more BTK disease
Outcomes between genders - no diff!
No safety apart from higher thrombosis female group
DM - much more calcified
Outcomes - no significant difference